1. Introduction
Infant and child mortality remains, in Senegal as in the rest of Sub-Saharan Africa, a key indicator for monitoring population health
| [1] | Reidpath DD, Allotey P. Infant mortality rate as an indicator of population health. J Epidemiol Community Health. 2003; 57(5): 344-6. |
[1]
. Each year, approximately 4.9 million children worldwide die before their first birthday, over 47% of whom die during the neonatal period
| [2] | UNICEF, WHO, World Bank, United Nations. Levels and Trends in Child Mortality - Report 2020. New York: UNICEF; 2020. |
[2]
. Although under-five mortality decreased by more than half between 1990 and 2015 as part of the Millennium Development Goals
| [3] | United Nations. The Millennium Development Goals Report 2015. New York: United Nations; 2015. |
[3]
, deep regional disparities persist. The risk of death before age one in the WHO African Region is more than six times higher than in the European Region
| [4] | World Health Organization. World Health Statistics 2021: monitoring health for the SDGs. Geneva: WHO; 2021. |
[4]
. In Sub-Saharan Africa (SSA), the infant and child mortality rate is estimated at 51 per 1,000 live births, with particularly marked excess mortality in West Africa (73 per 1,000 live births)
| [5] | Amare ZY, et al. Shared frailty survival analysis of under-five mortality in Sub-Saharan Africa. BMC Public Health. 2021. |
| [6] | Getaneh T, et al. Under-five mortality and its determinants in Sub-Saharan Africa: a multilevel analysis of recent Demographic and Health Surveys. BMC Public Health. 2025. |
[5, 6]
. These levels remain far from the Sustainable Development Goal 3.2 targets set for 2030: 12‰ for neonatal mortality and 25‰ for under-five mortality
| [7] | United Nations. Transforming our world: the 2030 Agenda for Sustainable Development. Resolution A/RES/70/1. New York: UN; 2015. |
[7]
.
The causes of this mortality are multidimensional. Direct factors such as malaria, respiratory infections, diarrhea, neonatal sepsis, prematurity, and malnutrition
| [8] | Black RE, Morris SS, Bryce J. Where and why are 10 million children dying every year? Lancet. 2003; 361(9376): 2226-34. |
[8]
are exacerbated by social determinants including low maternal education, household poverty, rural residence, and inadequate sanitation
| [9] | Dessie ZB, et al. Socioeconomic inequalities in infant mortality in Sub-Saharan Africa. BMC Public Health. 2024. |
| [10] | Ester PV, Torres A, Freire JM, Hernández V, Gil Á. Factors associated to infant mortality in Sub-Saharan Africa. J Public Health Africa. 2011; 2(2): e27. |
[9, 10]
. Beyond these individual factors, the organization of healthcare delivery itself constitutes a structural determinant of infant mortality. Longitudinal analyses of over 250,000 children in seven SSA countries showed that fees for vaccination (OR = 1.20) and delivery (OR = 1.11) were associated with significant excess infant and child mortality
| [11] | Torabi F, et al. Health systems context(s) and infant and child mortality in Sub-Saharan Africa, 1995-2015. Sci Rep. 2021. |
[11]
. In several West African countries, fewer than 50% of women give birth in the presence of skilled attendants
| [12] | Dadjo J, Omonaiye O, Yaya S. Health insurance coverage and access to child and maternal health services in West Africa: a systematic scoping review. Int Health. 2023; 15(6): 644-654.
https://doi.org/10.1093/inthealth/ihad071 |
[12]
, even though assisted deliveries substantially reduce the risk of neonatal death
| [12] | Dadjo J, Omonaiye O, Yaya S. Health insurance coverage and access to child and maternal health services in West Africa: a systematic scoping review. Int Health. 2023; 15(6): 644-654.
https://doi.org/10.1093/inthealth/ihad071 |
[12]
.
To address these challenges, several SSA countries have undertaken structural reforms of their health systems: free obstetric care policies, community-based health insurance, and strengthening of primary healthcare
| [13] | Novignon J, et al. Health expenditure and infant mortality in Sub-Saharan Africa. Health Econ Rev. 2020. |
| [14] | Alemayehu M, et al. Effective coverage of emergency obstetric and neonatal care services in Africa: a scoping review. Open Access Emerg Med. 2023. |
[13, 14]
. These mechanisms aim to remove financial and geographical barriers to healthcare access. However, their actual impact on infant and child mortality has not yet been systematically synthesized at the SSA level. Scoping reviews make it possible to map the extent and diversity of evidence in a heterogeneous field
| [15] | Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005; 8(1): 19-32. |
| [16] | Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018; 169(7): 467-73. |
[15, 16]
; this design therefore appears best suited to this objective. This scoping review aims to analyze the infant and child mortality risk factors documented in SSA between 2003 and 2023, with particular attention to the healthcare delivery components associated with variations in this mortality.
2. Methodology
2.1. Methodological Framework
This is a scoping review conducted according to the five-step methodological framework and aligned with PRISMA-ScR guidelines
| [15] | Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005; 8(1): 19-32. |
| [16] | Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018; 169(7): 467-73. |
| [17] | Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010; 5: 69. |
[15-17]
. This design was chosen to map a heterogeneous field where primary studies, evidence syntheses, and programmatic documents coexist
| [18] | Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil H. Chapter 10: Scoping Reviews. In: Aromataris E, Munn Z (eds). JBI Manual for Evidence Synthesis. Adelaide: JBI; 2020. |
[18]
.
2.2. Research Question
The research question was formulated according to the PCC (Population, Concept, Context) format recommended by the Joanna Briggs Institute (JBI)
| [18] | Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil H. Chapter 10: Scoping Reviews. In: Aromataris E, Munn Z (eds). JBI Manual for Evidence Synthesis. Adelaide: JBI; 2020. |
[18]
:
1) Population: Infants (0–11 months) and children under five years of age;
2) Concept: Infant mortality, risk factors, and components of healthcare delivery;
3) Context: Sub-Saharan African countries, period 2003–2023.
The guiding question is: “What are the documented risk factors for infant and child mortalityin Sub-Saharan Africa, and to what extent do healthcare delivery components contribute to them?”
2.3. Literature Search Strategy
Three databases and one search engine were queried: PubMed/MEDLINE, Web of Science, African Index Medicus, and Google Scholar. The search strategy was constructed using controlled MeSH terms and free-text words, combined according to Boolean operators AND/OR. The main terms used were: ("Infant Mortality" [MeSH] OR "Child Mortality" [MeSH] OR "Perinatal Mortality" [MeSH]) AND ("Risk Factors" [MeSH] OR "Cause of Death" [MeSH]) AND ("Health Services Accessibility" [MeSH] OR "Delivery of Health Care" [MeSH] OR "Primary Health Care" [MeSH]) AND ("Africa South of the Sahara" [MeSH] OR "Africa, Western" [MeSH]). The search was limited to publications from January 2003 to December 2023. A supplementary search of gray literature (WHO, UNICEF, World Bank, USAID reports) was conducted via Google Scholar and institutional websites. The references of included articles were also manually reviewed.
2.4. Eligibility Criteria
Studies were selected according to the following inclusion and exclusion criteria:
Table 1. Selection criteria.
Criteria | Inclusion | Exclusion |
Study type | Primary studies (cross-sectional, cohort, case-control, trials), systematic reviews, meta-analyses, institutional reports | Editorials, letters, opinions, isolated case studies |
Population | Infants (0–11 months) and children <5 years in Sub-Saharan Africa | Populations outside SSA or irrelevant age groups |
Language | French, English | Any other language |
Period | January 2003 – December 2023 | Publications prior to 2003 |
Research theme | Infant/neonatal mortality, at least one risk factor and one healthcare delivery component | Studies exclusively on maternal mortality without data on infant mortality |
Study Selection
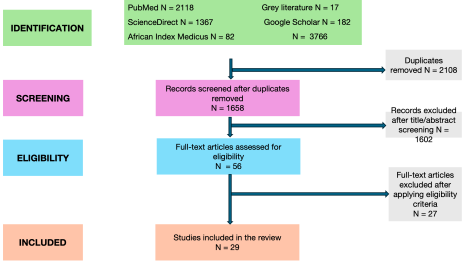
The literature search results were imported into Rayyan software for duplicate management and study selection. The selection was conducted in two independent and blinded phases: (i) title and abstract screening by two reviewers, followed by (ii) full-text reading of preselected articles. Disagreements were resolved by consensus or, if persistent, by arbitration with a third reviewer. The selection process is described according to the PRISMA-ScR flow diagram.
2.5. Data Extraction and Management
Data were extracted using a standardized form developed a priori and tested on five pilot articles. For each included study, the following information was collected: author(s), year and country of publication, study design, sample size, target population, risk factors explored, healthcare delivery components studied, main results, and reported mortality indicators. Two reviewers performed the extraction independently; disagreements were resolved through discussion.
2.6. Data Synthesis and Analysis
In accordance with JBI recommendations for scoping reviews
| [18] | Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil H. Chapter 10: Scoping Reviews. In: Aromataris E, Munn Z (eds). JBI Manual for Evidence Synthesis. Adelaide: JBI; 2020. |
[18]
, no formal methodological quality assessment of the studies was performed. The data underwent a structured narrative synthesis organized around major categories of risk factors. A descriptive summary table was produced to map the geographic distribution of studies, the designs used, and the most frequently documented healthcare delivery dimensions.
3. Results
3.1. Presentation of Study Selection
Figure 1. Flow diagram of study selection.
At the end of the PRISMA-ScR selection process, 29 documents were retained for the final synthesis. The selection includes 19 original scientific studies published in peer-reviewed journals and 10 contextual documents (institutional reports, communications, strategic and normative documents) covering more specifically the Senegalese and West African context. All of these documents cover the period 2003-2023 and provide an integrated mapping of infant and child mortality risk factors and healthcare delivery components in SSA.
3.2. Study Characteristics
The included studies show great methodological diversity. Observational designs dominate: cross-sectional studies from Demographic and Health Surveys (DHS)
| [19] | Ochieng Arunda M, Agardh A, Asamoah BO. Cesarean delivery and associated socioeconomic factors and neonatal survival outcome in Kenya and Tanzania: analysis of national survey data. Glob Health Action. 2020; 13(1): 1748403.
https://doi.org/10.1080/16549716.2020.1748403 |
| [20] | Adedini SA, Odimegwu C, Bamiwuye O, Fadeyibi O, De Wet N. Barriers to accessing health care in Nigeria: implications for child survival. Glob Health Action. 2014; 7: 23499.
https://doi.org/10.3402/gha.v7.23499 |
| [21] | Agence Nationale de la Statistique et de la Démographie (ANSD). Enquête Démographique et de Santé Continue du Senegal (EDS-C) 2017-2018. Dakar: ANSD; 2018. |
[19-21]
, prospective hospital cohorts
| [22] | Mujuru HA, Kambarami RA. Mortality within 24 hours of admission to the Paediatric Unit, Harare Central Hospital, Zimbabwe. Cent Afr J Med. 2012; 58(5-6): 17-22. |
| [23] | Agbeno EK, Osarfo J, Ashong J, Anane-Fenin B, Okai E, Ofori AA, Aliyu M, Opoku DA, Ken-Amoah S, Ashong JA, Soltani H. Determinants of preterm survival in a tertiary hospital in Ghana: a ten-year review. PLoS One. 2021; 16(1): e0246005.
https://doi.org/10.1371/journal.pone.0246005 |
[22, 23]
, case-control studies with social autopsy
| [24] | Preslar JP, Worrell MC, Kaiser R, Cain CJ, Samura S, Jambai A, Raghunathan PL, Clarke K, Goodman D, Christiansen-Lindquist L, Webb-Girard A, Kramer M, Breiman R. Effect of delays in maternal access to healthcare on neonatal mortality in Sierra Leone: a social autopsy case-control study at a Child Health and Mortality Prevention Surveillance (CHAMPS) site. Matern Child Health J. 2021; 25(8): 1326-1335.
https://doi.org/10.1007/s10995-021-03132-4 |
[24]
, perinatal audits using the three-delays model
| [25] | Musafili A, Persson LÅ, Baribwira C, Påfs J, Mulindwa PA, Essén B. Case review of perinatal deaths at hospitals in Kigali, Rwanda: perinatal audit with application of a three-delays analysis. BMC Pregnancy Childbirth. 2017; 17: 85.
https://doi.org/10.1186/s12884-017-1269-9 |
[25]
, verbal and social autopsies applied at community or national level
| [26] | Koffi AK, Mleme T, Nsona H, Banda B, Amouzou A, Kalter HD. Social autopsy of neonatal mortality suggests needed improvements in maternal and neonatal interventions in Balaka and Salima districts of Malawi. J Glob Health. 2015; 5(1): 010416. https://doi.org/10.7189/jogh.05.010416 |
| [27] | Källander K, Counihan H, Cerveau T, Mbofana F. Barriers on the pathway to survival for children dying from treatable illnesses in Inhambane province, Mozambique. J Glob Health. 2019; 9(1): 010809. https://doi.org/10.7189/jogh.09.010809 |
| [28] | Koffi AK, Kalter HD, Loveth EN, Quinley J, Monehin J, Black RE. Beyond causes of death: the social determinants of mortality among children aged 1-59 months in Nigeria from 2009 to 2013. PLoS One. 2017; 12(5): e0177025.
https://doi.org/10.1371/journal.pone.0177025 |
[26-28]
, multi-country ecological studies
| [29] | Alvarez JL, Gil R, Hernández V, Gil A. Factors associated with maternal mortality in Sub-Saharan Africa: an ecological study. BMC Public Health. 2009; 9: 462.
https://doi.org/10.1186/1471-2458-9-462 |
| [30] | Pretorius CE, Asare H, Kruger HS, Genuneit J, Siziba LP, Ricci C. Exclusive breastfeeding, child mortality, and economic cost in Sub-Saharan Africa. Pediatrics. 2021; 147(3): e2020030643. https://doi.org/10.1542/peds.2020-030643 |
[29, 30]
, and a hospital-community linked longitudinal study
| [31] | Veirum JE, Biai S, Jakobsen M, Sandström A, Hedegaard K, Kofoed PE, Aaby P, Sodemann M. Persisting high hospital and community childhood mortality in an urban setting in Guinea-Bissau. Acta Paediatr. 2007; 96(10): 1526-30.
https://doi.org/10.1111/j.1651-2227.2007.00467.x |
[31]
. Evidence syntheses complete this set: one systematic review
, one scoping review
| [12] | Dadjo J, Omonaiye O, Yaya S. Health insurance coverage and access to child and maternal health services in West Africa: a systematic scoping review. Int Health. 2023; 15(6): 644-654.
https://doi.org/10.1093/inthealth/ihad071 |
[12]
, and one exploratory review
| [33] | Ridde V, Morestin F. A scoping review of the literature on the abolition of user fees in health care services in Africa. Health Policy Plan. 2011; 26(1): 1-11.
https://doi.org/10.1093/heapol/czq021 |
[33]
. Quasi-experimental intervention evaluations
| [34] | Druetz T. Évaluation des effets de la gratuité des soins sur la morbidité, la mortalité et l'utilisation des services au Burkina Faso [thèse de doctorat]. Montréal: Université de Montréal; 2015. |
| [35] | Johri M, Ridde V, Heinmüller R, Haddad S. Estimation of maternal and child mortality one year after user-fee elimination: an impact evaluation and modelling study in Burkina Faso. Bull World Health Organ. 2014; 92(10): 706-15.
https://doi.org/10.2471/BLT.13.130609 |
| [36] | Ridde V, Haddad S, Heinmüller R. Improving equity by removing healthcare fees for children in Burkina Faso. J Epidemiol Community Health. 2013; 67(9): 751-7.
https://doi.org/10.1136/jech-2012-202080 |
[34-36]
and econometric time-series analyses
| [37] | Ndiaye M. Évaluation économétrique de l'impact de la politique de gratuité des soins sur la mortalité infantile et infanto-juvénile au Senegal (1980-2015). Dakar: IPAR; 2023. |
[37]
shed light on the impact of public policies. Finally, institutional and strategic documents (government reports, WHO, UNICEF, AFD, UN) structure the normative and programmatic framework
| [21] | Agence Nationale de la Statistique et de la Démographie (ANSD). Enquête Démographique et de Santé Continue du Senegal (EDS-C) 2017-2018. Dakar: ANSD; 2018. |
| [38] | UNICEF Senegal. Lancement de la politique de gratuité des soins pour les enfants de 0 à 5 ans – communiqué institutionnel. Dakar: UNICEF; octobre 2013. |
| [39] | Bureau d'Évaluation des Politiques Publiques (BEPP). Évaluation des politiques de gratuité des soins au Senegal. Dakar: Primature de la République du Senegal; 2011. |
| [40] | République du Senegal / OMS. Plan d'action national pour la réduction de la mortalité néonatale (2018-2022). Dakar: MSAS; 2018. |
| [41] | Organisation Mondiale de la Santé. Stratégie de coopération OMS-Senegal 2024-2028. Genève: OMS; 2024. |
| [42] | Comité des Droits Économiques, Sociaux et Culturels (CESCR-ONU). Observations finales concernant le troisième rapport périodique du Senegal. E/C.12/SEN/CO/3. Genève: ONU; 2019. |
| [43] | Agence Française de Développement (AFD). Appui à la politique de gratuité des soins de santé au Senegal – Document de programme. Paris: AFD; 2013. |
[21, 38-43]
.
The geographic coverage is broad: West Africa (Senegal, Mali, Burkina Faso, Nigeria, Niger, Ghana, Guinea-Bissau, Sierra Leone), East Africa (Kenya, Tanzania, Rwanda, Uganda), Southern Africa (Mozambique, Zimbabwe), and Central Africa (DRC). Reported mortality indicators include neonatal (0-28 days), post-neonatal, infant (<1 year), and under-five (<5 years) mortality, as well as, in some studies, perinatal mortality and maternal mortality as an indirect determinant of newborn survival
| [24] | Preslar JP, Worrell MC, Kaiser R, Cain CJ, Samura S, Jambai A, Raghunathan PL, Clarke K, Goodman D, Christiansen-Lindquist L, Webb-Girard A, Kramer M, Breiman R. Effect of delays in maternal access to healthcare on neonatal mortality in Sierra Leone: a social autopsy case-control study at a Child Health and Mortality Prevention Surveillance (CHAMPS) site. Matern Child Health J. 2021; 25(8): 1326-1335.
https://doi.org/10.1007/s10995-021-03132-4 |
| [25] | Musafili A, Persson LÅ, Baribwira C, Påfs J, Mulindwa PA, Essén B. Case review of perinatal deaths at hospitals in Kigali, Rwanda: perinatal audit with application of a three-delays analysis. BMC Pregnancy Childbirth. 2017; 17: 85.
https://doi.org/10.1186/s12884-017-1269-9 |
| [29] | Alvarez JL, Gil R, Hernández V, Gil A. Factors associated with maternal mortality in Sub-Saharan Africa: an ecological study. BMC Public Health. 2009; 9: 462.
https://doi.org/10.1186/1471-2458-9-462 |
[24, 25, 29]
. Target populations include newborns, premature infants
| [23] | Agbeno EK, Osarfo J, Ashong J, Anane-Fenin B, Okai E, Ofori AA, Aliyu M, Opoku DA, Ken-Amoah S, Ashong JA, Soltani H. Determinants of preterm survival in a tertiary hospital in Ghana: a ten-year review. PLoS One. 2021; 16(1): e0246005.
https://doi.org/10.1371/journal.pone.0246005 |
[23]
, children under five, and pregnant women in studies focusing on obstetric care
| [35] | Johri M, Ridde V, Heinmüller R, Haddad S. Estimation of maternal and child mortality one year after user-fee elimination: an impact evaluation and modelling study in Burkina Faso. Bull World Health Organ. 2014; 92(10): 706-15.
https://doi.org/10.2471/BLT.13.130609 |
[35]
(
Table 2).
3.3. Biological and Perinatal Factors
Direct causes of infant and child mortality remain dominated by infectious diseases and perinatal complications. Verbal and social autopsies conducted in Malawi
| [26] | Koffi AK, Mleme T, Nsona H, Banda B, Amouzou A, Kalter HD. Social autopsy of neonatal mortality suggests needed improvements in maternal and neonatal interventions in Balaka and Salima districts of Malawi. J Glob Health. 2015; 5(1): 010416. https://doi.org/10.7189/jogh.05.010416 |
[26]
and Niger
| [28] | Koffi AK, Kalter HD, Loveth EN, Quinley J, Monehin J, Black RE. Beyond causes of death: the social determinants of mortality among children aged 1-59 months in Nigeria from 2009 to 2013. PLoS One. 2017; 12(5): e0177025.
https://doi.org/10.1371/journal.pone.0177025 |
[28]
identify malaria, acute respiratory infections, and diarrheal diseases as the main biological causes, along with neonatal sepsis and malnutrition. The hospital-community linked study from Bissau
| [31] | Veirum JE, Biai S, Jakobsen M, Sandström A, Hedegaard K, Kofoed PE, Aaby P, Sodemann M. Persisting high hospital and community childhood mortality in an urban setting in Guinea-Bissau. Acta Paediatr. 2007; 96(10): 1526-30.
https://doi.org/10.1111/j.1651-2227.2007.00467.x |
[31]
confirms the predominance of malaria, ARI, and malnutrition among causes of in-hospital and community child mortality. In Inhambane (Mozambique), Källander et al. report a high proportion of deaths attributable to treatable causes (malaria, pneumonia, and diarrhea), the majority of which could have been prevented by early management
| [27] | Källander K, Counihan H, Cerveau T, Mbofana F. Barriers on the pathway to survival for children dying from treatable illnesses in Inhambane province, Mozambique. J Glob Health. 2019; 9(1): 010809. https://doi.org/10.7189/jogh.09.010809 |
[27]
.
Perinatal factors constitute the second major group of biological determinants. The ten-year retrospective study at Cape Coast Teaching Hospital (Ghana) shows that preterm infant survival is conditioned by gestational age, birth weight, and the occurrence of complications, with a clear gradient: the lower the gestational age, the higher the mortality
| [23] | Agbeno EK, Osarfo J, Ashong J, Anane-Fenin B, Okai E, Ofori AA, Aliyu M, Opoku DA, Ken-Amoah S, Ashong JA, Soltani H. Determinants of preterm survival in a tertiary hospital in Ghana: a ten-year review. PLoS One. 2021; 16(1): e0246005.
https://doi.org/10.1371/journal.pone.0246005 |
[23]
. The perinatal audit from Kigali (Rwanda) identifies perinatal asphyxia, prematurity, and low birth weight as major causes of perinatal death, a significant proportion of which were avoidable
| [25] | Musafili A, Persson LÅ, Baribwira C, Påfs J, Mulindwa PA, Essén B. Case review of perinatal deaths at hospitals in Kigali, Rwanda: perinatal audit with application of a three-delays analysis. BMC Pregnancy Childbirth. 2017; 17: 85.
https://doi.org/10.1186/s12884-017-1269-9 |
[25]
. The CHAMPS study in Sierra Leone reports that obstetric complications and prematurity are central to the genesis of neonatal mortality
| [24] | Preslar JP, Worrell MC, Kaiser R, Cain CJ, Samura S, Jambai A, Raghunathan PL, Clarke K, Goodman D, Christiansen-Lindquist L, Webb-Girard A, Kramer M, Breiman R. Effect of delays in maternal access to healthcare on neonatal mortality in Sierra Leone: a social autopsy case-control study at a Child Health and Mortality Prevention Surveillance (CHAMPS) site. Matern Child Health J. 2021; 25(8): 1326-1335.
https://doi.org/10.1007/s10995-021-03132-4 |
[24]
. Two specific determinants deserve emphasis: sickle cell disease, for which neonatal screening and early management significantly reduce mortality (demonstrated by the DRC pilot project
| [44] | Tshilolo L, Aissi LM, Lukusa D, et al. Neonatal screening for sickle cell anaemia in the Democratic Republic of the Congo: experience from a pioneer project. J Clin Pathol. 2008. |
[44]
), and exclusive breastfeeding, for which the ecological analysis with multi-country meta-regression (2000-2018) shows that it is associated with a substantial reduction in under-five mortality and considerable economic gains
| [30] | Pretorius CE, Asare H, Kruger HS, Genuneit J, Siziba LP, Ricci C. Exclusive breastfeeding, child mortality, and economic cost in Sub-Saharan Africa. Pediatrics. 2021; 147(3): e2020030643. https://doi.org/10.1542/peds.2020-030643 |
[30]
.
3.4. Maternal and Obstetric Factors
Maternal and obstetric determinants occupy a central place. Maternal education level, age at childbearing, and parity are consistently associated with child survival in multi-country DHS analyses
| [19] | Ochieng Arunda M, Agardh A, Asamoah BO. Cesarean delivery and associated socioeconomic factors and neonatal survival outcome in Kenya and Tanzania: analysis of national survey data. Glob Health Action. 2020; 13(1): 1748403.
https://doi.org/10.1080/16549716.2020.1748403 |
| [20] | Adedini SA, Odimegwu C, Bamiwuye O, Fadeyibi O, De Wet N. Barriers to accessing health care in Nigeria: implications for child survival. Glob Health Action. 2014; 7: 23499.
https://doi.org/10.3402/gha.v7.23499 |
[19, 20]
and in social autopsies
| [26] | Koffi AK, Mleme T, Nsona H, Banda B, Amouzou A, Kalter HD. Social autopsy of neonatal mortality suggests needed improvements in maternal and neonatal interventions in Balaka and Salima districts of Malawi. J Glob Health. 2015; 5(1): 010416. https://doi.org/10.7189/jogh.05.010416 |
| [28] | Koffi AK, Kalter HD, Loveth EN, Quinley J, Monehin J, Black RE. Beyond causes of death: the social determinants of mortality among children aged 1-59 months in Nigeria from 2009 to 2013. PLoS One. 2017; 12(5): e0177025.
https://doi.org/10.1371/journal.pone.0177025 |
[26, 28]
. The use of antenatal care (ANC) and the quality of its content appear as protective factors: the Kigali audit highlights that inadequate ANC is associated with excess perinatal deaths
| [25] | Musafili A, Persson LÅ, Baribwira C, Påfs J, Mulindwa PA, Essén B. Case review of perinatal deaths at hospitals in Kigali, Rwanda: perinatal audit with application of a three-delays analysis. BMC Pregnancy Childbirth. 2017; 17: 85.
https://doi.org/10.1186/s12884-017-1269-9 |
[25]
, and the Kenya-Tanzania DHS analysis shows a socioeconomic gradient in the use of obstetric care and cesarean section, with underuse among the poorest and overuse among the richest
| [19] | Ochieng Arunda M, Agardh A, Asamoah BO. Cesarean delivery and associated socioeconomic factors and neonatal survival outcome in Kenya and Tanzania: analysis of national survey data. Glob Health Action. 2020; 13(1): 1748403.
https://doi.org/10.1080/16549716.2020.1748403 |
[19]
.
The "three delays" model (decision, transport, care provision) helps to understand how maternal characteristics interact with healthcare delivery. The CHAMPS study shows that maternal delays contribute significantly to neonatal mortality
| [24] | Preslar JP, Worrell MC, Kaiser R, Cain CJ, Samura S, Jambai A, Raghunathan PL, Clarke K, Goodman D, Christiansen-Lindquist L, Webb-Girard A, Kramer M, Breiman R. Effect of delays in maternal access to healthcare on neonatal mortality in Sierra Leone: a social autopsy case-control study at a Child Health and Mortality Prevention Surveillance (CHAMPS) site. Matern Child Health J. 2021; 25(8): 1326-1335.
https://doi.org/10.1007/s10995-021-03132-4 |
[24]
. The Rwandan audit shows that Type 1 delays (decision to seek care) and Type 3 delays (quality of care at the facility) dominate among preventable perinatal deaths
| [25] | Musafili A, Persson LÅ, Baribwira C, Påfs J, Mulindwa PA, Essén B. Case review of perinatal deaths at hospitals in Kigali, Rwanda: perinatal audit with application of a three-delays analysis. BMC Pregnancy Childbirth. 2017; 17: 85.
https://doi.org/10.1186/s12884-017-1269-9 |
[25]
. In rural areas, the decision to seek care depends largely on social capital and community perceptions
| [27] | Källander K, Counihan H, Cerveau T, Mbofana F. Barriers on the pathway to survival for children dying from treatable illnesses in Inhambane province, Mozambique. J Glob Health. 2019; 9(1): 010809. https://doi.org/10.7189/jogh.09.010809 |
[27]
, and delayed care-seeking remains a major factor in excess mortality
| [27] | Källander K, Counihan H, Cerveau T, Mbofana F. Barriers on the pathway to survival for children dying from treatable illnesses in Inhambane province, Mozambique. J Glob Health. 2019; 9(1): 010809. https://doi.org/10.7189/jogh.09.010809 |
[27]
. The ecological analysis by Alvarez et al. on maternal mortality in SSA
| [29] | Alvarez JL, Gil R, Hernández V, Gil A. Factors associated with maternal mortality in Sub-Saharan Africa: an ecological study. BMC Public Health. 2009; 9: 462.
https://doi.org/10.1186/1471-2458-9-462 |
[29]
(an indirect but powerful determinant of newborn survival), confirms that the density of skilled human resources and coverage of maternal indicators (ANC, assisted delivery) are negatively associated with maternal mortality. Finally, Pretorius et al. emphasize the protective role of early-initiated exclusive breastfeeding
| [30] | Pretorius CE, Asare H, Kruger HS, Genuneit J, Siziba LP, Ricci C. Exclusive breastfeeding, child mortality, and economic cost in Sub-Saharan Africa. Pediatrics. 2021; 147(3): e2020030643. https://doi.org/10.1542/peds.2020-030643 |
[30]
.
3.5. Socioeconomic and Environmental Factors
Socioeconomic determinants are cross-cutting and powerful. Poverty, low maternal education, and rural residence are systematically associated with increased mortality in DHS analyses
| [19] | Ochieng Arunda M, Agardh A, Asamoah BO. Cesarean delivery and associated socioeconomic factors and neonatal survival outcome in Kenya and Tanzania: analysis of national survey data. Glob Health Action. 2020; 13(1): 1748403.
https://doi.org/10.1080/16549716.2020.1748403 |
| [20] | Adedini SA, Odimegwu C, Bamiwuye O, Fadeyibi O, De Wet N. Barriers to accessing health care in Nigeria: implications for child survival. Glob Health Action. 2014; 7: 23499.
https://doi.org/10.3402/gha.v7.23499 |
[19, 20]
, social autopsies
| [26] | Koffi AK, Mleme T, Nsona H, Banda B, Amouzou A, Kalter HD. Social autopsy of neonatal mortality suggests needed improvements in maternal and neonatal interventions in Balaka and Salima districts of Malawi. J Glob Health. 2015; 5(1): 010416. https://doi.org/10.7189/jogh.05.010416 |
| [28] | Koffi AK, Kalter HD, Loveth EN, Quinley J, Monehin J, Black RE. Beyond causes of death: the social determinants of mortality among children aged 1-59 months in Nigeria from 2009 to 2013. PLoS One. 2017; 12(5): e0177025.
https://doi.org/10.1371/journal.pone.0177025 |
[26, 28]
, the systematic review by Rutherford et al.
, and Senegalese contextual studies
| [45] | Fall M. Inégalités sociales d'utilisation des soins de santé maternelle et infantile au Senegal après la politique de gratuité: décomposition d'inégalités. Dakar: IPAR; 2023. |
[45]
. The UN CESCR report documents a major inequality in Senegal: infant and child mortality stands at 63% in rural areas versus 43% in urban areas
| [42] | Comité des Droits Économiques, Sociaux et Culturels (CESCR-ONU). Observations finales concernant le troisième rapport périodique du Senegal. E/C.12/SEN/CO/3. Genève: ONU; 2019. |
[42]
. The equity analysis by Fall in Senegal shows that the free care policy increased overall healthcare utilization but paradoxically widened pro-rich inequalities in ANC and consultations
| [45] | Fall M. Inégalités sociales d'utilisation des soins de santé maternelle et infantile au Senegal après la politique de gratuité: décomposition d'inégalités. Dakar: IPAR; 2023. |
[45]
. The scoping review by Dadjo et al. on West Africa confirms that although health insurance improves access to maternal and child health services, coverage remains very low and unevenly distributed
| [12] | Dadjo J, Omonaiye O, Yaya S. Health insurance coverage and access to child and maternal health services in West Africa: a systematic scoping review. Int Health. 2023; 15(6): 644-654.
https://doi.org/10.1093/inthealth/ihad071 |
[12]
.
Environmental factors, although less systematically reported, play a confirmed role. Access to safe water, sanitation, and housing quality (WASH) are identified as determinants in the Malawi social autopsy
| [26] | Koffi AK, Mleme T, Nsona H, Banda B, Amouzou A, Kalter HD. Social autopsy of neonatal mortality suggests needed improvements in maternal and neonatal interventions in Balaka and Salima districts of Malawi. J Glob Health. 2015; 5(1): 010416. https://doi.org/10.7189/jogh.05.010416 |
[26]
and the Rutherford systematic review
. Ndiaye shows that in Senegal, improved access to safe water, coupled with the availability of antimalarials, explains a substantial part of the decline in under-five mortality between 1980 and 2015, whereas free care alone proved insufficient to transform this indicator in the short term
| [37] | Ndiaye M. Évaluation économétrique de l'impact de la politique de gratuité des soins sur la mortalité infantile et infanto-juvénile au Senegal (1980-2015). Dakar: IPAR; 2023. |
[37]
. Social capital and community support networks also appear as modulating factors in the care-seeking pathway
| [27] | Källander K, Counihan H, Cerveau T, Mbofana F. Barriers on the pathway to survival for children dying from treatable illnesses in Inhambane province, Mozambique. J Glob Health. 2019; 9(1): 010809. https://doi.org/10.7189/jogh.09.010809 |
[27]
.
3.6. Contribution of Healthcare Delivery
3.6.1. Geographic and Organizational Accessibility, and Continuity of Care
Geographic and organizational accessibility of healthcare delivery is a primary structural determinant. Multivariate DHS analyses show that distance to facilities, transport availability, and shortage of qualified personnel are associated with excess under-five mortality
| [20] | Adedini SA, Odimegwu C, Bamiwuye O, Fadeyibi O, De Wet N. Barriers to accessing health care in Nigeria: implications for child survival. Glob Health Action. 2014; 7: 23499.
https://doi.org/10.3402/gha.v7.23499 |
[20]
. The systematic review by Rutherford et al. concludes there is a robust and recurrent association between access barriers (geographic and financial) and under-five mortality in SSA
. Social autopsies confirm this relationship in Niger
| [28] | Koffi AK, Kalter HD, Loveth EN, Quinley J, Monehin J, Black RE. Beyond causes of death: the social determinants of mortality among children aged 1-59 months in Nigeria from 2009 to 2013. PLoS One. 2017; 12(5): e0177025.
https://doi.org/10.1371/journal.pone.0177025 |
[28]
and Malawi
| [26] | Koffi AK, Mleme T, Nsona H, Banda B, Amouzou A, Kalter HD. Social autopsy of neonatal mortality suggests needed improvements in maternal and neonatal interventions in Balaka and Salima districts of Malawi. J Glob Health. 2015; 5(1): 010416. https://doi.org/10.7189/jogh.05.010416 |
[26]
.
The continuum of care around hospitalization appears fragile. In Bissau, despite hospitalizations, community mortality remains high: many children die at home without reaching the hospital, and those who are discharged have excess post-hospitalization mortality
| [31] | Veirum JE, Biai S, Jakobsen M, Sandström A, Hedegaard K, Kofoed PE, Aaby P, Sodemann M. Persisting high hospital and community childhood mortality in an urban setting in Guinea-Bissau. Acta Paediatr. 2007; 96(10): 1526-30.
https://doi.org/10.1111/j.1651-2227.2007.00467.x |
[31]
. In Harare, Mujuru et al. report that the majority of in-hospital deaths occur within 24 hours of admission, with very significant pre-admission delays
| [22] | Mujuru HA, Kambarami RA. Mortality within 24 hours of admission to the Paediatric Unit, Harare Central Hospital, Zimbabwe. Cent Afr J Med. 2012; 58(5-6): 17-22. |
[22]
. The mobilization of community health workers (CHWs) in Mozambique improves care-seeking, but their coverage remains partial and financial barriers persist
| [27] | Källander K, Counihan H, Cerveau T, Mbofana F. Barriers on the pathway to survival for children dying from treatable illnesses in Inhambane province, Mozambique. J Glob Health. 2019; 9(1): 010809. https://doi.org/10.7189/jogh.09.010809 |
[27]
. The three-delays model, applied in Rwanda
| [25] | Musafili A, Persson LÅ, Baribwira C, Påfs J, Mulindwa PA, Essén B. Case review of perinatal deaths at hospitals in Kigali, Rwanda: perinatal audit with application of a three-delays analysis. BMC Pregnancy Childbirth. 2017; 17: 85.
https://doi.org/10.1186/s12884-017-1269-9 |
[25]
and Sierra Leone
| [24] | Preslar JP, Worrell MC, Kaiser R, Cain CJ, Samura S, Jambai A, Raghunathan PL, Clarke K, Goodman D, Christiansen-Lindquist L, Webb-Girard A, Kramer M, Breiman R. Effect of delays in maternal access to healthcare on neonatal mortality in Sierra Leone: a social autopsy case-control study at a Child Health and Mortality Prevention Surveillance (CHAMPS) site. Matern Child Health J. 2021; 25(8): 1326-1335.
https://doi.org/10.1007/s10995-021-03132-4 |
[24]
, demonstrates that the quality of facility-based care (3rd delay) is as critical as the decision or transport delay.
3.6.2. Healthcare Financing and Free Care/Exemption Policies
Financial barriers constitute a major and recurring obstacle to access to pediatric care. DHS analyses
| [19] | Ochieng Arunda M, Agardh A, Asamoah BO. Cesarean delivery and associated socioeconomic factors and neonatal survival outcome in Kenya and Tanzania: analysis of national survey data. Glob Health Action. 2020; 13(1): 1748403.
https://doi.org/10.1080/16549716.2020.1748403 |
| [20] | Adedini SA, Odimegwu C, Bamiwuye O, Fadeyibi O, De Wet N. Barriers to accessing health care in Nigeria: implications for child survival. Glob Health Action. 2014; 7: 23499.
https://doi.org/10.3402/gha.v7.23499 |
[19, 20]
, social autopsies
| [26] | Koffi AK, Mleme T, Nsona H, Banda B, Amouzou A, Kalter HD. Social autopsy of neonatal mortality suggests needed improvements in maternal and neonatal interventions in Balaka and Salima districts of Malawi. J Glob Health. 2015; 5(1): 010416. https://doi.org/10.7189/jogh.05.010416 |
| [28] | Koffi AK, Kalter HD, Loveth EN, Quinley J, Monehin J, Black RE. Beyond causes of death: the social determinants of mortality among children aged 1-59 months in Nigeria from 2009 to 2013. PLoS One. 2017; 12(5): e0177025.
https://doi.org/10.1371/journal.pone.0177025 |
[26, 28]
, the systematic review
, and the Bissau community study
| [31] | Veirum JE, Biai S, Jakobsen M, Sandström A, Hedegaard K, Kofoed PE, Aaby P, Sodemann M. Persisting high hospital and community childhood mortality in an urban setting in Guinea-Bissau. Acta Paediatr. 2007; 96(10): 1526-30.
https://doi.org/10.1111/j.1651-2227.2007.00467.x |
[31]
all converge in identifying the cost of care (direct fees, informal payments, indirect costs) as a factor in excess mortality.
Free care and exemption policies aimed at removing these barriers have been extensively evaluated in SSA. The exploratory review by Ridde and Morestin, on fee abolition in Africa, reports a substantial increase in healthcare utilization and a documented reduction in child morbidity and mortality, particularly in Sahelian countries
| [33] | Ridde V, Morestin F. A scoping review of the literature on the abolition of user fees in health care services in Africa. Health Policy Plan. 2011; 26(1): 1-11.
https://doi.org/10.1093/heapol/czq021 |
[33]
. The quasi-experimental evaluation by Ridde, Haddad, and Heinmüller in Burkina Faso demonstrates that removing user fees for children improves equity in access to care
| [36] | Ridde V, Haddad S, Heinmüller R. Improving equity by removing healthcare fees for children in Burkina Faso. J Epidemiol Community Health. 2013; 67(9): 751-7.
https://doi.org/10.1136/jech-2012-202080 |
[36]
. Druetz's thesis on Burkina Faso estimates that free care combined with quality improvement could have saved between 14,000 and 19,000 child lives, although morbidity did not improve significantly
| [34] | Druetz T. Évaluation des effets de la gratuité des soins sur la morbidité, la mortalité et l'utilisation des services au Burkina Faso [thèse de doctorat]. Montréal: Université de Montréal; 2015. |
[34]
. In Mali and Senegal, exemption from cesarean section fees is associated with increased use of obstetric procedures, with expected benefits for neonatal survival
| [35] | Johri M, Ridde V, Heinmüller R, Haddad S. Estimation of maternal and child mortality one year after user-fee elimination: an impact evaluation and modelling study in Burkina Faso. Bull World Health Organ. 2014; 92(10): 706-15.
https://doi.org/10.2471/BLT.13.130609 |
[35]
.
In Senegal, the policy arsenal combines free care for children aged 0-5 years launched in October 2013
| [38] | UNICEF Senegal. Lancement de la politique de gratuité des soins pour les enfants de 0 à 5 ans – communiqué institutionnel. Dakar: UNICEF; octobre 2013. |
[38]
, the national neonatal mortality reduction plan
| [40] | République du Senegal / OMS. Plan d'action national pour la réduction de la mortalité néonatale (2018-2022). Dakar: MSAS; 2018. |
[40]
, the strengthening of Universal Health Coverage (UHC)
| [41] | Organisation Mondiale de la Santé. Stratégie de coopération OMS-Senegal 2024-2028. Genève: OMS; 2024. |
[41]
, and financial support from donors
| [43] | Agence Française de Développement (AFD). Appui à la politique de gratuité des soins de santé au Senegal – Document de programme. Paris: AFD; 2013. |
[43]
. Available evaluations paint a mixed picture. BEPP documents increased healthcare utilization following the implementation of free care policies, while identifying residual non-financial barriers
| [39] | Bureau d'Évaluation des Politiques Publiques (BEPP). Évaluation des politiques de gratuité des soins au Senegal. Dakar: Primature de la République du Senegal; 2011. |
[39]
. DHS-Continuing 2017-2018 confirms a downward trend in infant and child mortality indicators post-2013
| [21] | Agence Nationale de la Statistique et de la Démographie (ANSD). Enquête Démographique et de Santé Continue du Senegal (EDS-C) 2017-2018. Dakar: ANSD; 2018. |
[21]
. Ndiaye's econometric analysis over the period 1980-2015 concludes that high-impact interventions – distribution of antimalarials and improved access to safe water – are the main factors associated with the decline in under-five mortality, with free care alone proving insufficient
| [37] | Ndiaye M. Évaluation économétrique de l'impact de la politique de gratuité des soins sur la mortalité infantile et infanto-juvénile au Senegal (1980-2015). Dakar: IPAR; 2023. |
[37]
. Pouye reports mixed effects of free care on child malnutrition
| [46] | Pouye R. Effets de la gratuité des soins sur la dénutrition de l'enfant au Senegal: analyse quantitative. Communication présentée au Colloque annuel IPAR, Dakar; 2023. |
[46]
, while Fall highlights that the policy, although globally positive for utilization, has increased pro-rich inequalities in ANC and consultations
| [45] | Fall M. Inégalités sociales d'utilisation des soins de santé maternelle et infantile au Senegal après la politique de gratuité: décomposition d'inégalités. Dakar: IPAR; 2023. |
[45]
. The UN CESCR emphasizes that the effectiveness of free care must be strengthened, particularly in rural areas where infant and child mortality inequalities persist
| [42] | Comité des Droits Économiques, Sociaux et Culturels (CESCR-ONU). Observations finales concernant le troisième rapport périodique du Senegal. E/C.12/SEN/CO/3. Genève: ONU; 2019. |
[42]
. Finally, the scoping review by Dadjo et al. on West Africa shows that health insurance and exemptions increase access to maternal and child health services, but that coverage remains very low at the regional level
| [12] | Dadjo J, Omonaiye O, Yaya S. Health insurance coverage and access to child and maternal health services in West Africa: a systematic scoping review. Int Health. 2023; 15(6): 644-654.
https://doi.org/10.1093/inthealth/ihad071 |
[12]
, a finding confirmed by the WHO-Senegal UHC strategic framework 2024-2028
| [41] | Organisation Mondiale de la Santé. Stratégie de coopération OMS-Senegal 2024-2028. Genève: OMS; 2024. |
[41]
.
In summary, the available evidence converges on a triple observation:
(i) Financial barriers remain a robust determinant of infant and child mortality in SSA;
(ii) Free care and exemption policies improve healthcare utilization and save lives when supported by parallel quality improvement;
(iii) Their impact on mortality is modulated by the persistence of non-financial barriers (distance, quality, socioeconomic and environmental inequalities) and by the risk of paradoxically increasing pro-rich inequalities in the absence of targeted measures.
Table 2. Characteristics of included studies.
N° | First author | Year | Ref | Study design | N | Target age group |
1 | Ridde V, Haddad S, Heinmüller R | 2013 | | [36] | Ridde V, Haddad S, Heinmüller R. Improving equity by removing healthcare fees for children in Burkina Faso. J Epidemiol Community Health. 2013; 67(9): 751-7.
https://doi.org/10.1136/jech-2012-202080 |
[36] | Scientific article (quasi-experimental) | Burkina Faso | <5 years |
2 | Pouye R | 2023 | | [46] | Pouye R. Effets de la gratuité des soins sur la dénutrition de l'enfant au Senegal: analyse quantitative. Communication présentée au Colloque annuel IPAR, Dakar; 2023. |
[46] | Conference communication (quantitative analysis) | Senegalese data | <5 years |
3 | Ndiaye M | 2023 | | [37] | Ndiaye M. Évaluation économétrique de l'impact de la politique de gratuité des soins sur la mortalité infantile et infanto-juvénile au Senegal (1980-2015). Dakar: IPAR; 2023. |
[37] | Econometric analysis (time series 1980-2015) | Aggregated Senegal data | 0-5 years |
4 | Fall M | 2023 | | [45] | Fall M. Inégalités sociales d'utilisation des soins de santé maternelle et infantile au Senegal après la politique de gratuité: décomposition d'inégalités. Dakar: IPAR; 2023. |
[45] | Quantitative analysis (inequality decomposition) | Household surveys (Senegal) | <5 years |
5 | Republic of Senegal/WHO | 2018 | | [40] | République du Senegal / OMS. Plan d'action national pour la réduction de la mortalité néonatale (2018-2022). Dakar: MSAS; 2018. |
[40] | National action plan | National coverage | Neonatal |
6 | UNICEF Senegal | 2013 | | [38] | UNICEF Senegal. Lancement de la politique de gratuité des soins pour les enfants de 0 à 5 ans – communiqué institutionnel. Dakar: UNICEF; octobre 2013. |
[38] | Institutional report | ≈2.5 million children <5 years (target population) | 0-5 years |
7 | Druetz T | 2015 | | [34] | Druetz T. Évaluation des effets de la gratuité des soins sur la morbidité, la mortalité et l'utilisation des services au Burkina Faso [thèse de doctorat]. Montréal: Université de Montréal; 2015. |
[34] | PhD thesis (intervention pre-post) | Burkina Faso population | <5 years |
8 | BEPP | 2011 | | [39] | Bureau d'Évaluation des Politiques Publiques (BEPP). Évaluation des politiques de gratuité des soins au Senegal. Dakar: Primature de la République du Senegal; 2011. |
[39] | Government evaluation report | Prior national coverage | 0-5 years + pregnant women |
9 | UN CESCR | 2019 | | [42] | Comité des Droits Économiques, Sociaux et Culturels (CESCR-ONU). Observations finales concernant le troisième rapport périodique du Senegal. E/C.12/SEN/CO/3. Genève: ONU; 2019. |
[42] | UN report (concluding observations) | National (Senegal) | <5 years |
10 | Johri M | 2014 | | [35] | Johri M, Ridde V, Heinmüller R, Haddad S. Estimation of maternal and child mortality one year after user-fee elimination: an impact evaluation and modelling study in Burkina Faso. Bull World Health Organ. 2014; 92(10): 706-15.
https://doi.org/10.2471/BLT.13.130609 |
[35] | Scientific article (quasi-experimental) | Mali & Senegal populations | Pregnant women + newborns |
11 | ANSD | 2018 | | [21] | Agence Nationale de la Statistique et de la Démographie (ANSD). Enquête Démographique et de Santé Continue du Senegal (EDS-C) 2017-2018. Dakar: ANSD; 2018. |
[21] | National survey (DHS-Continuing 2017-2018) | National sample 2017-18 | <5 years |
12 | Alvarez JL | 2009 | | [29] | Alvarez JL, Gil R, Hernández V, Gil A. Factors associated with maternal mortality in Sub-Saharan Africa: an ecological study. BMC Public Health. 2009; 9: 462.
https://doi.org/10.1186/1471-2458-9-462 |
[29] | Ecological study (SSA countries) | SSA countries (aggregated analysis) | Women of childbearing age (maternal mortality) |
13 | Källander K | 2019 | | [27] | Källander K, Counihan H, Cerveau T, Mbofana F. Barriers on the pathway to survival for children dying from treatable illnesses in Inhambane province, Mozambique. J Glob Health. 2019; 9(1): 010809. https://doi.org/10.7189/jogh.09.010809 |
[27] | Mixed study (caregiver interviews, autopsy) | Caregivers of deceased children <5 in 2015 (Inhambane) | <5 years |
14 | Agbeno EK | 2021 | | [23] | Agbeno EK, Osarfo J, Ashong J, Anane-Fenin B, Okai E, Ofori AA, Aliyu M, Opoku DA, Ken-Amoah S, Ashong JA, Soltani H. Determinants of preterm survival in a tertiary hospital in Ghana: a ten-year review. PLoS One. 2021; 16(1): e0246005.
https://doi.org/10.1371/journal.pone.0246005 |
[23] | Retrospective hospital study (10 years) | Preterm infants in SCBU (Cape Coast) | Preterm infants |
15 | Mujuru HA | 2012 | | [22] | Mujuru HA, Kambarami RA. Mortality within 24 hours of admission to the Paediatric Unit, Harare Central Hospital, Zimbabwe. Cent Afr J Med. 2012; 58(5-6): 17-22. |
[22] | Prospective hospital cohort | Admitted patients (pediatric unit, Harare) | Children (not strictly specified in abstract) |
16 | Tshilolo L | 2008 | | [44] | Tshilolo L, Aissi LM, Lukusa D, et al. Neonatal screening for sickle cell anaemia in the Democratic Republic of the Congo: experience from a pioneer project. J Clin Pathol. 2008. |
[44] | Narrative/systematic review (pilot programs) | Pilot screening programs (DRC + SSA) | Neonatal |
17 | Pretorius CE | 2021 | | [30] | Pretorius CE, Asare H, Kruger HS, Genuneit J, Siziba LP, Ricci C. Exclusive breastfeeding, child mortality, and economic cost in Sub-Saharan Africa. Pediatrics. 2021; 147(3): e2020030643. https://doi.org/10.1542/peds.2020-030643 |
[30] | Ecological analysis + meta-regression (2000-2018) | SSA countries (World Bank) | <5 years |
18 | Adedini SA | 2014 | | [20] | Adedini SA, Odimegwu C, Bamiwuye O, Fadeyibi O, De Wet N. Barriers to accessing health care in Nigeria: implications for child survival. Glob Health Action. 2014; 7: 23499.
https://doi.org/10.3402/gha.v7.23499 |
[20] | Multivariate DHS analysis 2008 Nigeria | NAHS 2008 – children <5 years | <5 years |
19 | Koffi AK | 2017 | | [26] | Koffi AK, Mleme T, Nsona H, Banda B, Amouzou A, Kalter HD. Social autopsy of neonatal mortality suggests needed improvements in maternal and neonatal interventions in Balaka and Salima districts of Malawi. J Glob Health. 2015; 5(1): 010416. https://doi.org/10.7189/jogh.05.010416 |
[26] | Verbal and social autopsy (retrospective) | Deaths <5 years (3 districts, 2007–2010) | <5 years |
20 | Koffi AK | 2016 | | [28] | Koffi AK, Kalter HD, Loveth EN, Quinley J, Monehin J, Black RE. Beyond causes of death: the social determinants of mortality among children aged 1-59 months in Nigeria from 2009 to 2013. PLoS One. 2017; 12(5): e0177025.
https://doi.org/10.1371/journal.pone.0177025 |
[28] | Verbal and social autopsy (national) | Deaths <5 years (Niger national sample 2012) | <5 years |
21 | Veirum JE | 2007 | | [31] | Veirum JE, Biai S, Jakobsen M, Sandström A, Hedegaard K, Kofoed PE, Aaby P, Sodemann M. Persisting high hospital and community childhood mortality in an urban setting in Guinea-Bissau. Acta Paediatr. 2007; 96(10): 1526-30.
https://doi.org/10.1111/j.1651-2227.2007.00467.x |
[31] | Longitudinal hospital-community linked study (DSS linkage) | 6 years of hospital data + community cohort | <5 years |
22 | Rutherford ME | 2010 | | Systematic review | Studies included in SSA (not specified in abstract) | <5 years |
23 | WHO | 2024 | | [41] | Organisation Mondiale de la Santé. Stratégie de coopération OMS-Senegal 2024-2028. Genève: OMS; 2024. |
[41] | Strategic document (CCS WHO-Senegal) | National | NA |
24 | Preslar JP | 2021 | | [24] | Preslar JP, Worrell MC, Kaiser R, Cain CJ, Samura S, Jambai A, Raghunathan PL, Clarke K, Goodman D, Christiansen-Lindquist L, Webb-Girard A, Kramer M, Breiman R. Effect of delays in maternal access to healthcare on neonatal mortality in Sierra Leone: a social autopsy case-control study at a Child Health and Mortality Prevention Surveillance (CHAMPS) site. Matern Child Health J. 2021; 25(8): 1326-1335.
https://doi.org/10.1007/s10995-021-03132-4 |
[24] | Case-control (social autopsy – CHAMPS) | Cases (neonatal deaths) + controls (survivors), CHAMPS site | Newborns (0–28 d) |
25 | Musafili A | 2017 | | [25] | Musafili A, Persson LÅ, Baribwira C, Påfs J, Mulindwa PA, Essén B. Case review of perinatal deaths at hospitals in Kigali, Rwanda: perinatal audit with application of a three-delays analysis. BMC Pregnancy Childbirth. 2017; 17: 85.
https://doi.org/10.1186/s12884-017-1269-9 |
[25] | Hospital perinatal audit (3-delays model) | Perinatal deaths (2 Kigali hospitals, Jul 2012–May 2013) | Perinatal (22 weeks–7 d) |
26 | Dadjo J | 2023 | | [12] | Dadjo J, Omonaiye O, Yaya S. Health insurance coverage and access to child and maternal health services in West Africa: a systematic scoping review. Int Health. 2023; 15(6): 644-654.
https://doi.org/10.1093/inthealth/ihad071 |
[12] | Scoping review (PRISMA-ScR) | Included studies in West Africa | Mother-child |
27 | Ochieng Arunda M | 2020 | | [19] | Ochieng Arunda M, Agardh A, Asamoah BO. Cesarean delivery and associated socioeconomic factors and neonatal survival outcome in Kenya and Tanzania: analysis of national survey data. Glob Health Action. 2020; 13(1): 1748403.
https://doi.org/10.1080/16549716.2020.1748403 |
[19] | Cross-sectional DHS analysis (logistic regression) | DHS Kenya & Tanzania (live births) | Newborns |
28 | Ridde V, Morestin F | 2011 | | [33] | Ridde V, Morestin F. A scoping review of the literature on the abolition of user fees in health care services in Africa. Health Policy Plan. 2011; 26(1): 1-11.
https://doi.org/10.1093/heapol/czq021 |
[33] | Exploratory literature review | African studies on fee abolition | General population (focus mother-child) |
29 | AFD | 2013 | | [43] | Agence Française de Développement (AFD). Appui à la politique de gratuité des soins de santé au Senegal – Document de programme. Paris: AFD; 2013. |
[43] | Program document (donor) | 4 Sahelian countries (including Senegal) | <5 years |
N° | Biological & perinatal factors | Maternal factors | Socioeconomic factors | Environmental factors | Healthcare delivery: Accessibility | Healthcare delivery: Financing & costs | Mortality Indicator |
1 | NA | NA | Equity | NA | Healthcare utilization | User fee removal for children | Equity of access (mortality proxy) |
2 | Malnutrition | NA | Inequalities | NA | Healthcare utilization | Free care policies | Malnutrition/morbidity (intermediate outcome) |
3 | NA | NA | NA | Safe water (exposure) | NA | Free care policy | Under-5 mortality |
4 | NA | NA | Social inequalities in healthcare utilization | NA | Healthcare utilization (ANC, consultations) | Exemption/free care policy | Healthcare utilization (mortality proxy) |
5 | NA | NA | NA | NA | Neonatal mortality reduction strategies | Includes free care | Neonatal mortality (programmatic target) |
6 | NA | NA | National coverage | NA | Free care package: consultation, vaccination, hospitalization | Free care – launch Oct. 2013 | Objective: reduce under-5 mortality (programmatic target) |
7 | Child morbidity, stunting | NA | NA | NA | Healthcare utilization | Free care + quality improvement | Infant and child mortality (estimated lives saved) |
8 | NA | Pregnant women | Poverty | NA | Documented increased utilization | Free care – impact evaluation | MDGs, poverty, utilization |
9 | NA | NA | Urban-rural inequalities | NA | Effectiveness of free care; inequalities | Free care | Rural IM 63% vs urban IM 43% |
10 | NA | Delivery (cesarean) | NA | NA | Obstetric service utilization | Cesarean section fee exemption | Cesarean utilization (neonatal survival proxy) |
11 | NA | NA | NA | NA | NA | Post-2013 free care data | Infant and child mortality (intermediate values) |
12 | NA | Maternal indicators (ANC, assisted delivery) | GDP, health spending | NA | Human resources, facility density | Health spending (% of GDP) | Maternal mortality (outcome) |
13 | Treatable causes (malaria, pneumonia, diarrhea) | Delayed care-seeking, social capital | Social capital, poverty | NA | CHWs – coverage and use | Costs related to care; financial barriers | Under-5 mortality |
14 | Gestational age, birth weight, complications | ANC, complications | NA | NA | SCBU (Cape Coast Teaching Hospital) | Costs of neonatal care (implicit) | Preterm survival / neonatal mortality |
15 | Illness duration, severity at admission | Care-seeking behavior | NA | NA | Delay in care-seeking and care provision | Cost mentioned as barrier to early care-seeking | In-hospital mortality <24h |
16 | Sickle cell disease (exposure) | NA | Poverty | NA | Neonatal screening and clinical follow-up | Cost and resources for screening | Sickle cell mortality/morbidity |
17 | Exclusive breastfeeding (EBF) | Breastfeeding, nutrition | Poverty, GDP | NA | NA | Economic cost (secondary outcome) | Under-5 mortality + economic cost |
18 | NA | Education, maternal age | Income, residence | NA | Distance, transport, staff shortage | Cost of care, prohibitive fees | Under-5 mortality |
19 | Pneumonia, diarrhea, malaria (biological causes) | Education, care-seeking behavior | Poverty, residence | WASH, housing | Distance, transport | Cost of care, household financing | Under-5 mortality |
20 | Malaria, pneumonia, diarrhea | Care-seeking, education | Poverty, residence | NA | Distance, availability | Cost of care, financing | Under-5 mortality |
21 | Hospital causes (malaria, ARI, malnutrition) | NA | Urban residence (Bissau) | NA | Pediatric hospitalization rate; hospital coverage | Cost of care mentioned as barrier | Community mortality + in-hospital under-5 mortality |
22 | Various (synthesis) | Various | Poverty, education | WASH, housing | Distance, availability, quality | Cost of care (recurrent barrier) | Under-5 mortality |
23 | NA | NA | NA | NA | UHC (strengthening) | UHC | NA |
24 | Obstetric complications, prematurity | Maternal delays (decision/transport/care – 3 delays) | Low maternal education, poverty (barrier) | NA | Delays in access to maternal care (3 delays) | Financial barriers to care access | Neonatal mortality |
25 | Perinatal asphyxia, prematurity, low birth weight | Inadequate ANC, obstetric complications, parity | Poverty, maternal education | NA | Delays 1/2/3 (care-seeking, transport, care); quality of care | Financial barriers (OOP) cited in all 3 delays | Perinatal mortality |
26 | NA | Maternal service utilization | Insurance status, poverty | NA | Mother-child service coverage | Health insurance/UHC, fee exemption | Access to mother-child care (intermediate outcome) |
27 | Delivery mode (cesarean) | Maternal age, parity, ANC | Wealth index, education, residence | NA | Obstetric care utilization; access to cesarean | Health insurance/UHC; OOP | Neonatal mortality |
28 | NA | NA | Poverty | NA | Healthcare utilization | User fee abolition | Utilization + infant morbidity/mortality |
29 | NA | NA | NA | NA | Financial access to care | EUR 8M (I3S); CFAF 1.8B Senegal 2013 | Access to care for <5 years (target) |
NA: NON AVAILABLE
4. Discussion
Based on 29 documents published between 2003 and 2023, this scoping review mapped the risk factors for infant and child mortality and the components of healthcare delivery in Sub-Saharan Africa, with a particular focus on Senegal. Four major groups of determinants emerge: biological and perinatal factors, maternal and obstetric factors, socioeconomic and environmental determinants, and healthcare delivery, considered in its dual dimensions of organizational accessibility and financing. Comparison with the existing literature.
Our results are broadly consistent with the international body of literature on the social determinants of child health. The convergence between social autopsies
| [26] | Koffi AK, Mleme T, Nsona H, Banda B, Amouzou A, Kalter HD. Social autopsy of neonatal mortality suggests needed improvements in maternal and neonatal interventions in Balaka and Salima districts of Malawi. J Glob Health. 2015; 5(1): 010416. https://doi.org/10.7189/jogh.05.010416 |
| [27] | Källander K, Counihan H, Cerveau T, Mbofana F. Barriers on the pathway to survival for children dying from treatable illnesses in Inhambane province, Mozambique. J Glob Health. 2019; 9(1): 010809. https://doi.org/10.7189/jogh.09.010809 |
| [28] | Koffi AK, Kalter HD, Loveth EN, Quinley J, Monehin J, Black RE. Beyond causes of death: the social determinants of mortality among children aged 1-59 months in Nigeria from 2009 to 2013. PLoS One. 2017; 12(5): e0177025.
https://doi.org/10.1371/journal.pone.0177025 |
[26-28]
, hospital audits
| [22] | Mujuru HA, Kambarami RA. Mortality within 24 hours of admission to the Paediatric Unit, Harare Central Hospital, Zimbabwe. Cent Afr J Med. 2012; 58(5-6): 17-22. |
| [25] | Musafili A, Persson LÅ, Baribwira C, Påfs J, Mulindwa PA, Essén B. Case review of perinatal deaths at hospitals in Kigali, Rwanda: perinatal audit with application of a three-delays analysis. BMC Pregnancy Childbirth. 2017; 17: 85.
https://doi.org/10.1186/s12884-017-1269-9 |
[22, 25]
, DHS analyses
| [19] | Ochieng Arunda M, Agardh A, Asamoah BO. Cesarean delivery and associated socioeconomic factors and neonatal survival outcome in Kenya and Tanzania: analysis of national survey data. Glob Health Action. 2020; 13(1): 1748403.
https://doi.org/10.1080/16549716.2020.1748403 |
| [20] | Adedini SA, Odimegwu C, Bamiwuye O, Fadeyibi O, De Wet N. Barriers to accessing health care in Nigeria: implications for child survival. Glob Health Action. 2014; 7: 23499.
https://doi.org/10.3402/gha.v7.23499 |
[19, 20]
, and evidence syntheses
| [12] | Dadjo J, Omonaiye O, Yaya S. Health insurance coverage and access to child and maternal health services in West Africa: a systematic scoping review. Int Health. 2023; 15(6): 644-654.
https://doi.org/10.1093/inthealth/ihad071 |
| [32] | Rutherford ME, Mulholland K, Hill PC. How access to health care relates to under-five mortality in Sub-Saharan Africa: systematic review. Trop Med Int Health. 2010; 15(5): 508-19. https://doi.org/10.1111/j.1365-3156.2010.02497.x |
| [33] | Ridde V, Morestin F. A scoping review of the literature on the abolition of user fees in health care services in Africa. Health Policy Plan. 2011; 26(1): 1-11.
https://doi.org/10.1093/heapol/czq021 |
[12, 32, 33]
reinforces the robustness of the reported associations. Three points nevertheless deserve particular attention.
First, the financial dimension of healthcare access is systematically documented, both in community studies
| [26] | Koffi AK, Mleme T, Nsona H, Banda B, Amouzou A, Kalter HD. Social autopsy of neonatal mortality suggests needed improvements in maternal and neonatal interventions in Balaka and Salima districts of Malawi. J Glob Health. 2015; 5(1): 010416. https://doi.org/10.7189/jogh.05.010416 |
| [27] | Källander K, Counihan H, Cerveau T, Mbofana F. Barriers on the pathway to survival for children dying from treatable illnesses in Inhambane province, Mozambique. J Glob Health. 2019; 9(1): 010809. https://doi.org/10.7189/jogh.09.010809 |
| [28] | Koffi AK, Kalter HD, Loveth EN, Quinley J, Monehin J, Black RE. Beyond causes of death: the social determinants of mortality among children aged 1-59 months in Nigeria from 2009 to 2013. PLoS One. 2017; 12(5): e0177025.
https://doi.org/10.1371/journal.pone.0177025 |
| [31] | Veirum JE, Biai S, Jakobsen M, Sandström A, Hedegaard K, Kofoed PE, Aaby P, Sodemann M. Persisting high hospital and community childhood mortality in an urban setting in Guinea-Bissau. Acta Paediatr. 2007; 96(10): 1526-30.
https://doi.org/10.1111/j.1651-2227.2007.00467.x |
[26-28, 31]
and in population-based analyses
| [12] | Dadjo J, Omonaiye O, Yaya S. Health insurance coverage and access to child and maternal health services in West Africa: a systematic scoping review. Int Health. 2023; 15(6): 644-654.
https://doi.org/10.1093/inthealth/ihad071 |
| [19] | Ochieng Arunda M, Agardh A, Asamoah BO. Cesarean delivery and associated socioeconomic factors and neonatal survival outcome in Kenya and Tanzania: analysis of national survey data. Glob Health Action. 2020; 13(1): 1748403.
https://doi.org/10.1080/16549716.2020.1748403 |
| [20] | Adedini SA, Odimegwu C, Bamiwuye O, Fadeyibi O, De Wet N. Barriers to accessing health care in Nigeria: implications for child survival. Glob Health Action. 2014; 7: 23499.
https://doi.org/10.3402/gha.v7.23499 |
[12, 19, 20]
and reviews
| [32] | Rutherford ME, Mulholland K, Hill PC. How access to health care relates to under-five mortality in Sub-Saharan Africa: systematic review. Trop Med Int Health. 2010; 15(5): 508-19. https://doi.org/10.1111/j.1365-3156.2010.02497.x |
| [33] | Ridde V, Morestin F. A scoping review of the literature on the abolition of user fees in health care services in Africa. Health Policy Plan. 2011; 26(1): 1-11.
https://doi.org/10.1093/heapol/czq021 |
[32, 33]
. This convergence justifies the priority given to financial protection through free care policies, exemptions, and universal health coverage
| [36] | Ridde V, Haddad S, Heinmüller R. Improving equity by removing healthcare fees for children in Burkina Faso. J Epidemiol Community Health. 2013; 67(9): 751-7.
https://doi.org/10.1136/jech-2012-202080 |
| [38] | UNICEF Senegal. Lancement de la politique de gratuité des soins pour les enfants de 0 à 5 ans – communiqué institutionnel. Dakar: UNICEF; octobre 2013. |
| [41] | Organisation Mondiale de la Santé. Stratégie de coopération OMS-Senegal 2024-2028. Genève: OMS; 2024. |
[36, 38, 41]
. However, intervention evaluations conducted in Burkina Faso
| [34] | Druetz T. Évaluation des effets de la gratuité des soins sur la morbidité, la mortalité et l'utilisation des services au Burkina Faso [thèse de doctorat]. Montréal: Université de Montréal; 2015. |
| [35] | Johri M, Ridde V, Heinmüller R, Haddad S. Estimation of maternal and child mortality one year after user-fee elimination: an impact evaluation and modelling study in Burkina Faso. Bull World Health Organ. 2014; 92(10): 706-15.
https://doi.org/10.2471/BLT.13.130609 |
| [36] | Ridde V, Haddad S, Heinmüller R. Improving equity by removing healthcare fees for children in Burkina Faso. J Epidemiol Community Health. 2013; 67(9): 751-7.
https://doi.org/10.1136/jech-2012-202080 |
[34-36]
and the Senegalese econometric analysis
| [37] | Ndiaye M. Évaluation économétrique de l'impact de la politique de gratuité des soins sur la mortalité infantile et infanto-juvénile au Senegal (1980-2015). Dakar: IPAR; 2023. |
[37]
show that free care alone is a necessary but insufficient lever: its effect on mortality depends on a concurrent improvement in care quality and the removal of non-financial barriers.
Second, the issue of equity appears central. Inequality analyses in Senegal
| [45] | Fall M. Inégalités sociales d'utilisation des soins de santé maternelle et infantile au Senegal après la politique de gratuité: décomposition d'inégalités. Dakar: IPAR; 2023. |
[45]
and UN CESCR observations
| [42] | Comité des Droits Économiques, Sociaux et Culturels (CESCR-ONU). Observations finales concernant le troisième rapport périodique du Senegal. E/C.12/SEN/CO/3. Genève: ONU; 2019. |
[42]
show that universal free care policies can paradoxically widen pro-rich inequalities in healthcare utilization when non-financial barriers (distance, perceived quality, social capital) persist. This phenomenon, also found by Ochieng Arunda et al. in Kenya and Tanzania for cesarean sections
| [19] | Ochieng Arunda M, Agardh A, Asamoah BO. Cesarean delivery and associated socioeconomic factors and neonatal survival outcome in Kenya and Tanzania: analysis of national survey data. Glob Health Action. 2020; 13(1): 1748403.
https://doi.org/10.1080/16549716.2020.1748403 |
[19]
and by Dadjo et al. at the West African level
| [12] | Dadjo J, Omonaiye O, Yaya S. Health insurance coverage and access to child and maternal health services in West Africa: a systematic scoping review. Int Health. 2023; 15(6): 644-654.
https://doi.org/10.1093/inthealth/ihad071 |
[12]
, argues for policies that actively target disadvantaged households and territories, rather than uniform free care. This approach aligns with the broader literature on progressive universal health coverage.
Third, the role of non-medical structural factors in reducing infant and child mortality deserves emphasis. Ndiaye's Senegalese time series analysis
| [37] | Ndiaye M. Évaluation économétrique de l'impact de la politique de gratuité des soins sur la mortalité infantile et infanto-juvénile au Senegal (1980-2015). Dakar: IPAR; 2023. |
[37]
identifies access to safe water and the availability of antimalarials as the main drivers of the decline observed between 1980 and 2015. This finding supports multisectoral approaches linking health, water, sanitation and hygiene, nutrition
| [30] | Pretorius CE, Asare H, Kruger HS, Genuneit J, Siziba LP, Ricci C. Exclusive breastfeeding, child mortality, and economic cost in Sub-Saharan Africa. Pediatrics. 2021; 147(3): e2020030643. https://doi.org/10.1542/peds.2020-030643 |
[30]
, and social protection
| [43] | Agence Française de Développement (AFD). Appui à la politique de gratuité des soins de santé au Senegal – Document de programme. Paris: AFD; 2013. |
[43]
.
4.1. Implications for Senegal and Francophone West Africa
From a programmatic perspective, the assessment of the free care policy launched in 2013
| [38] | UNICEF Senegal. Lancement de la politique de gratuité des soins pour les enfants de 0 à 5 ans – communiqué institutionnel. Dakar: UNICEF; octobre 2013. |
[38]
and the National Neonatal Mortality Reduction Plan
| [40] | République du Senegal / OMS. Plan d'action national pour la réduction de la mortalité néonatale (2018-2022). Dakar: MSAS; 2018. |
[40]
call for strengthening the quality and equity components, beyond the financial dimension alone. The findings from BEPP
| [39] | Bureau d'Évaluation des Politiques Publiques (BEPP). Évaluation des politiques de gratuité des soins au Senegal. Dakar: Primature de la République du Senegal; 2011. |
[39]
, ANSD
| [21] | Agence Nationale de la Statistique et de la Démographie (ANSD). Enquête Démographique et de Santé Continue du Senegal (EDS-C) 2017-2018. Dakar: ANSD; 2018. |
[21]
, and the UN CESCR report
| [42] | Comité des Droits Économiques, Sociaux et Culturels (CESCR-ONU). Observations finales concernant le troisième rapport périodique du Senegal. E/C.12/SEN/CO/3. Genève: ONU; 2019. |
[42]
converge in highlighting the persistence of an urban-rural gradient (63% vs 43%), which calls for differentiated territorial coverage strategies.
From a strategic standpoint, the implementation of the WHO-Senegal Cooperation Strategy 2024-2028
| [41] | Organisation Mondiale de la Santé. Stratégie de coopération OMS-Senegal 2024-2028. Genève: OMS; 2024. |
[41]
and the support from donors such as AFD
| [43] | Agence Française de Développement (AFD). Appui à la politique de gratuité des soins de santé au Senegal – Document de programme. Paris: AFD; 2013. |
[43]
offer a window of opportunity to reorient investment toward high-impact interventions for mortality reduction: quality emergency obstetric and neonatal care, neonatal screening for sickle cell disease
| [44] | Tshilolo L, Aissi LM, Lukusa D, et al. Neonatal screening for sickle cell anaemia in the Democratic Republic of the Congo: experience from a pioneer project. J Clin Pathol. 2008. |
[44]
, promotion of exclusive breastfeeding
| [30] | Pretorius CE, Asare H, Kruger HS, Genuneit J, Siziba LP, Ricci C. Exclusive breastfeeding, child mortality, and economic cost in Sub-Saharan Africa. Pediatrics. 2021; 147(3): e2020030643. https://doi.org/10.1542/peds.2020-030643 |
[30]
, strengthening of community health workers and task shifting for integrated management of childhood illnesses, and consolidation of UHC financing within a progressive and equitable framework
| [12] | Dadjo J, Omonaiye O, Yaya S. Health insurance coverage and access to child and maternal health services in West Africa: a systematic scoping review. Int Health. 2023; 15(6): 644-654.
https://doi.org/10.1093/inthealth/ihad071 |
| [41] | Organisation Mondiale de la Santé. Stratégie de coopération OMS-Senegal 2024-2028. Genève: OMS; 2024. |
| [45] | Fall M. Inégalités sociales d'utilisation des soins de santé maternelle et infantile au Senegal après la politique de gratuité: décomposition d'inégalités. Dakar: IPAR; 2023. |
[12, 41, 45]
.
On the research front, several gaps remain to be filled: impact evaluations of free care that go beyond healthcare utilization, i.e., focusing on mortality and morbidity, using robust quasi-experimental designs
| [34] | Druetz T. Évaluation des effets de la gratuité des soins sur la morbidité, la mortalité et l'utilisation des services au Burkina Faso [thèse de doctorat]. Montréal: Université de Montréal; 2015. |
| [37] | Ndiaye M. Évaluation économétrique de l'impact de la politique de gratuité des soins sur la mortalité infantile et infanto-juvénile au Senegal (1980-2015). Dakar: IPAR; 2023. |
[34, 37]
; qualitative studies on care-seeking pathways in rural Senegal, following the three-delays framework
| [24] | Preslar JP, Worrell MC, Kaiser R, Cain CJ, Samura S, Jambai A, Raghunathan PL, Clarke K, Goodman D, Christiansen-Lindquist L, Webb-Girard A, Kramer M, Breiman R. Effect of delays in maternal access to healthcare on neonatal mortality in Sierra Leone: a social autopsy case-control study at a Child Health and Mortality Prevention Surveillance (CHAMPS) site. Matern Child Health J. 2021; 25(8): 1326-1335.
https://doi.org/10.1007/s10995-021-03132-4 |
| [25] | Musafili A, Persson LÅ, Baribwira C, Påfs J, Mulindwa PA, Essén B. Case review of perinatal deaths at hospitals in Kigali, Rwanda: perinatal audit with application of a three-delays analysis. BMC Pregnancy Childbirth. 2017; 17: 85.
https://doi.org/10.1186/s12884-017-1269-9 |
[24, 25]
; action research on the equity of UHC coverage and its articulation with mandatory health insurance
| [12] | Dadjo J, Omonaiye O, Yaya S. Health insurance coverage and access to child and maternal health services in West Africa: a systematic scoping review. Int Health. 2023; 15(6): 644-654.
https://doi.org/10.1093/inthealth/ihad071 |
| [45] | Fall M. Inégalités sociales d'utilisation des soins de santé maternelle et infantile au Senegal après la politique de gratuité: décomposition d'inégalités. Dakar: IPAR; 2023. |
[12, 45]
; and production of local data on causes of neonatal death using CHAMPS-type social autopsies
| [24] | Preslar JP, Worrell MC, Kaiser R, Cain CJ, Samura S, Jambai A, Raghunathan PL, Clarke K, Goodman D, Christiansen-Lindquist L, Webb-Girard A, Kramer M, Breiman R. Effect of delays in maternal access to healthcare on neonatal mortality in Sierra Leone: a social autopsy case-control study at a Child Health and Mortality Prevention Surveillance (CHAMPS) site. Matern Child Health J. 2021; 25(8): 1326-1335.
https://doi.org/10.1007/s10995-021-03132-4 |
| [27] | Källander K, Counihan H, Cerveau T, Mbofana F. Barriers on the pathway to survival for children dying from treatable illnesses in Inhambane province, Mozambique. J Glob Health. 2019; 9(1): 010809. https://doi.org/10.7189/jogh.09.010809 |
| [28] | Koffi AK, Kalter HD, Loveth EN, Quinley J, Monehin J, Black RE. Beyond causes of death: the social determinants of mortality among children aged 1-59 months in Nigeria from 2009 to 2013. PLoS One. 2017; 12(5): e0177025.
https://doi.org/10.1371/journal.pone.0177025 |
[24, 27, 28]
.
4.2. Strengths and Limitations
This study has several strengths. The rigorous application of the PRISMA-ScR methodology, followed by the structured retention of 29 documents, ensures both scientific and programmatic coverage of the field. The diversity of included study designs facilitates triangulation of results. The systematic integration of Senegalese contextual documents anchors the discussion in the national reality.
Several limitations must nevertheless be acknowledged. First, a scoping review neither aims to formally assess the methodological quality of included studies nor to produce pooled effect estimates; the comparison of association magnitudes therefore remains descriptive. Second, the heterogeneity of study designs, populations, and mortality indicators limits quantitative synthesis. The inclusion of programmatic and institutional documents
| [38] | UNICEF Senegal. Lancement de la politique de gratuité des soins pour les enfants de 0 à 5 ans – communiqué institutionnel. Dakar: UNICEF; octobre 2013. |
| [39] | Bureau d'Évaluation des Politiques Publiques (BEPP). Évaluation des politiques de gratuité des soins au Senegal. Dakar: Primature de la République du Senegal; 2011. |
| [40] | République du Senegal / OMS. Plan d'action national pour la réduction de la mortalité néonatale (2018-2022). Dakar: MSAS; 2018. |
| [41] | Organisation Mondiale de la Santé. Stratégie de coopération OMS-Senegal 2024-2028. Genève: OMS; 2024. |
| [42] | Comité des Droits Économiques, Sociaux et Culturels (CESCR-ONU). Observations finales concernant le troisième rapport périodique du Senegal. E/C.12/SEN/CO/3. Genève: ONU; 2019. |
| [43] | Agence Française de Développement (AFD). Appui à la politique de gratuité des soins de santé au Senegal – Document de programme. Paris: AFD; 2013. |
[38-43]
, while relevant to the context, adds additional heterogeneity that must be considered in interpretation. Finally, the restriction to publications in French and English indexed in the searched databases may have excluded relevant work published in other languages; a selection bias cannot therefore be completely ruled out.