Abstract
This case report details the occurrence of adrenal insufficiency in a 46-year-old male undergoing anti-tuberculosis (TB) treatment. The patient developed clinical symptoms indicative of adrenal insufficiency on the fourth day following the initiation of anti-Tuberculosis treatment which consisted of rifampicin, a key component of the TB treatment regimen. Initial symptoms at fourth day of treatment included postural dizziness, fatigue, nausea, and abdominal pain. His biochemical investigations revealed hypoglycemia, hyperkalemia, mild metabolic acidosis, and a disproportionately low random cortisol level during the acute presentation. A diagnosis of rifampicin-induced adrenal insufficiency was strongly suspected, supported by clinical presentation and the temporal relationship to therapy initiation. The patient was subsequently transferred to the intensive care unit and his condition improved only after initiating, administering of hydrocortisone and discontinuing rifampicin therapy. Following stabilization, an alternative anti-TB regimen excluding rifampicin was introduced. The patient showed gradual clinical improvement with hydrocortisone therapy and continued TB treatment. The report discusses clinical presentation, diagnostic evaluation, management, and the importance of recognizing this potential life-threatening adverse effect providing insight into the critical need for increased awareness and early recognition of adrenal insufficiency as a rare but potentially life-threatening complication of anti-tuberculosis therapy, extending the importance to guiding clinical vigilance and treatment protocols. This case serves an important reference and supports the routine monitoring of adrenal function during rifampicin therapy to guide future clinical practice.
|
Published in
|
Science Journal of Public Health (Volume 13, Issue 1)
|
|
DOI
|
10.11648/j.sjph.20251301.12
|
|
Page(s)
|
12-16 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Tuberculosis, Adrenal Insufficiency, Rifampicin Treatment
1. Introduction
Tuberculosis (TB) continues to pose a significant global health challenge, requiring prolonged treatment with combination antibiotic regimen including isoniazid, rifampicin, pyrazinamide, and ethambutol. Rifampicin, in particular, plays a crucial role due to its potent bactericidal activity against Mycobacterium tuberculosis.
Adrenal insufficiency is a condition characterized by the inadequate production of cortisol, a vital steroid hormone required for stress response, metabolism, and electrolyte regulation. This disorder arises from reduced cortisol secretion by the adrenal glands, which may result from various underlying causes.
Adrenal insufficiency in tuberculosis is commonly reported by the infiltration of the pituitary or adrenal glands by Mycobacterium tuberculosis, however rifampin has also been suggested as a causative agent.
Rifampicin is a potent inducer of liver cytochrome P450IIIA enzyme which plays key role in the metabolism of various drugs, dietary compounds, and steroid hormones. As a result, rifampicin can increase the metabolism of adrenal steroid hormones particularly cortisol, potentially leading to adrenal insufficiency
| [1] | Karam, M. C., Merhbi, S. S., & Ghalayini, W. M. (2013). Rifampicin-induced adrenal insufficiency. International Journal of Tuberculosis and Lung Disease, 17(6), 836-838. |
[1]
.
Prevalence data on rifampicin-induced adrenal insufficiency is limited. However, this condition is particularly documented in patients who are undergoing long-term rifampicin therapy, where the cumulative effects on adrenal function can be profound
| [1] | Karam, M. C., Merhbi, S. S., & Ghalayini, W. M. (2013). Rifampicin-induced adrenal insufficiency. International Journal of Tuberculosis and Lung Disease, 17(6), 836-838. |
[1]
. Adrenal insufficiency is also recognized in patients with concurrent use of other medications that influence adrenal function or those with pre-existing adrenal disease
| [9] | Yee, T. W.; Mathews, G. J.; Subramaniam, S. D..; Abdullah, N. R. A.; Merican, N. S. Y. A. RIFAMPIN-INDUCED ADRENAL CRISIS. J ASEAN Fed Endocr Soc 2024, 39, 13. |
[9]
.
Adrenal insufficiency can present nonspecific symptoms such as fatigue, weight loss, hypotension, and hyperpigmentation, which may complicate its diagnosis in patients already undergoing treatment for TB. However, understanding and recognizing this condition is crucial for timely diagnosis and management, as untreated adrenal insufficiency can lead to severe complications, including adrenal crisis. We report an unusual case of life-threatening adrenal insufficiency due to the usage of rifampicin in pulmonary TB patients.
2. Case Summary
A 46-year-old male presented with a three-month history of productive cough, progressive exertional dyspnea, evening pyrexia, fatigue and weight loss. Patient’s initial sputum Acid-fast bacillus (AFB) was positive. He was diagnosed as a case of smear positive pulmonary TB and started on anti TB treatment as new case according to Sri Lankan guideline. Anti-Tuberculosis treatment regimen consisted of Isoniazid, Rifampicin, Pyrazinamide, and Ethambutol and drug doses were adjusted according to his body weight.
On the 4th day of anti- TB treatment, patient complained of postural dizziness, nausea, fatigue and right ileac fossa pain.
Upon On clinical examination, he was ill- looking, dehydrated but afebrile and had there was bilateral ankle edema. Blood pressure was 70/50 mmHg, heart rate of 110 beats per minute with elevated Jugular venous pressure. There was a loud pulmonary second heart sound. His trachea deviated to the left side and auscultation of the chest revealed defuse coarse crepitations on the left lung. Oxygen saturation was 92% on room air. Abdominal and neurological examinations were normal.
In light of the patient's acute deterioration, several differential diagnoses were considered. Acute myocardial infarction was a key consideration, given the sudden onset of his symptoms. The possibility of deep vein thrombosis leading to acute massive pulmonary embolism, particularly due to his recent period of immobilization during hospitalization and the presence of a loud pulmonary second heart sound was another considered possibility. Septic shock was considered in the differential diagnosis due to the underlying secondary bacterial infection contributing to his worsening condition. Strong consideration of adrenal failure, taking into account his clinical history of pulmonary TB which raises the possibility of adrenal involvement was. Furthermore rifampicin- induced adrenal insufficiency was supported considering total clinical picture over other possibilities.
3. Laboratory Investigations
Based on the above differential diagnosis, we conducted the following investigations were conducted.
1) An electrocardiogram (ECG) demonstrated sinus tachycardia with right axis deviation, P- pulmonale and T wave inversion in V1- V4 leads.
Table 1. Hematological Investigations.
White blood cells | 8.6×109/L (<11×109/L) |
Neutrophils | 76% |
lymphocytes | 21% |
Eosinophils | 2% |
Hemoglobin | 9.2 g/dL (12-16 g/dl) |
Platelets | 224×109/L (150-450×109/L) |
C reactive protein | 36 mg/L (<6 mg/L) |
Erythrocyte sedimentation rate (ESR) | 84 mm/ 1st hour |
Table 2. Biochemical Investigations.
Serum creatinine | 102 µmol/L (54–110 µmol/L) |
Blood urea | 15.4 mmol/L (2.5–6.5 mmol/L) |
Serum sodium | 129 mmol/L (135–146 mmol/L) |
Serum potassium | 5.7 mmol/L (3.5–5.3 mmol/L) |
Serum chloride | 100 mmol/L (96–106 mmol/L) |
Random blood sugar | 64 mg/dl |
Troponin I | 286 ng/L (High) |
D- dimer levels | 1.2 mg/l (<0.5 mg/l) |
Random cortisol level | 322 nmol/L (250–650 nmol/L) |
Table 3. Arterial blood gas analysis revealed metabolic acidosis.
pH | 7.32 |
PaO2 | 69 mmhg |
PaCO2 | 34 mmhg |
HCO-3 | 18 mmol/l (24 mmol/l) |
Lactate | mmol/l (<1) |
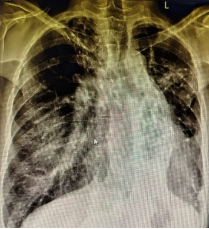
a) Trachea was deviated to left.
b) Elongated heart.
c) Left side extensive volume loss with fibrosis, scaring, bronchiectasis.
d) Pleural thickening in the lower zones.
e) Right sided lower zone shadows with consolidations.
f) Compensatory hyper expansion of the right lung.
g) Bilateral upper zone scattered calcifications with fibrosis.
h) Prominent pulmonary vessels.
2) 2D Echocardiogram showed mild to moderate pulmonary hypertension, mild right atrium and ventricular dilatation with normal left ventricular functions.
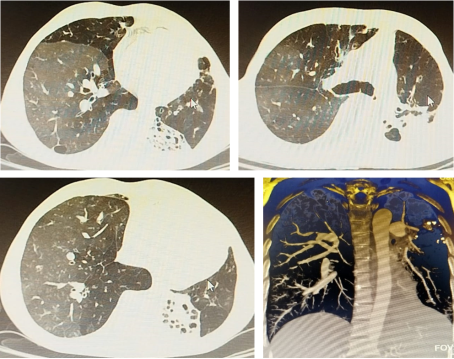
Pulmonary windows of the computed tomography pulmonary angiography (CTPA) showed mediastinal deviation and volume loss in the left lobe. There were reticulations and fibrosis in the upper lobe of the left lung. Evidence of bronchiectasis, multiple cavities and collapses of left lingula lobe and lower lobes. scattered nodules and consolidations were noted in the right lung. CTPA showed no filling defects in the major pulmonary arteries.
3) Ultrasound scan (USS)- Abdomen normal with preserved adrenal architecture
Figure 2. CTPA with pulmonary windows.
4. Treatment
Based on the clinical presentation and laboratory findings, a diagnosis of adrenal insufficiency was made. Given the temporal relationship with the initiation of anti-TB therapy and the known enzyme-inducing properties of rifampicin, rifampicin-induced adrenal insufficiency was strongly suspected.
The patient was initially resuscitated with crystalloid boluses at a dose of 20 milliliters per kilogram along with intravenous hydrocortisone at a dose of one hundred milligrams. Despite these interventions, hypotension persisted and did not respond adequately to fluid resuscitation. As a result, vasopressor support was initiated with intravenous norepinephrine delivered via a central venous line. Broad-spectrum antibiotics, intravenous meropenem, were administered with microbiological concurrence to cover potential infections. Blood glucose levels were closely monitored considering the potential risk of hypoglycemia. Antitubercular therapy was temporarily withheld, and the patient was subsequently transferred to the intensive care unit for close monitoring.
Upon transfer to the intensive care unit, the patient was monitored closely for hemodynamic stability and response to treatment. Over the next few days, blood pressure gradually improved, allowing for a reduction in vasopressor support. We initiated intravenous hydrocortisone at a dose of fifty milligrams every six hours for three days, then transitioned to a physiological replacement regimen of oral hydrocortisone 10 milligrams in the morning, 5 milligrams at noon, and 5 milligrams in the evening.
Outcome and follow-up
The patient was educated about the importance of adherence to treatment and the potential side effects of medications. A multidisciplinary approach was implemented to ensure comprehensive care, including input from endocrinology specialist. To assess adrenal insufficiency further, we arranged a computed tomography scan of the abdomen and plasma metyrapone testing.
Regular follow-ups were scheduled to monitor adrenal function and the management of his pulmonary tuberculosis. The findings prompted the initiation of an alternative anti TB treatment regimen tailored to his needs. Rifampicin was withheld permanently and alternative anti- TB treatment regimen with Isoniazid, Ethambutol, Pyrazinamide and Levofloxacin was started.
5. Discussion
The management of Pulmonary TB patients would be done with close monitoring and vigilance to detect common, unusual complications due to disease itself, treatment side effects and other unrelated complications. Change of clinical status of these patients would be evaluated with holistic approach to ascertain definitive diagnosis.
Anti-tuberculosis (TB) medications are associated with a diverse spectrum of adverse effects that can impact multiple organ systems, most notably the liver, kidneys, and gastrointestinal tract. These drug-related complications can significantly contribute to the clinical deterioration of a patient’s condition if not promptly identified and managed [3].
Among these drug-related side effects, *Rifampicin-induced adrenal insufficiency* is a rare but important complication. Although uncommon, this condition can lead to severe outcomes if not promptly identified and treated. Early recognition is essential to avoid life-threatening consequences
| [4] | Jonatan D Lindh, Jekaterina Patrova, R Louise Rushworth, Buster Mannheimer, Henrik Falhammar, Tuberculosis of Adrenal Glands—A Population-based Case-control Study, Journal of the Endocrine Society, Volume 7, Issue 5, May 2023, bvad047, https://doi.org/10.1210/jendso/bvad047 |
| [5] | Gupta S, Ansari MAM, Gupta AK, Chaudhary P, Bansal LK. Current Approach for Diagnosis and Treatment of Adrenal Tuberculosis-Our Experience and Review of Literature. Surg J (N Y). 2022 Mar 3; 8(1): e92-e97. https://doi.org/10.1055/s-0042-1743523 |
[4, 5]
.
Rifampicin is a potent inducer of the cytochrome P450 enzyme system, which significantly accelerates the metabolism of steroid hormones. The mechanism underlying rifampicin-induced adrenal insufficiency is the enhanced hepatic clearance of endogenous cortisol
| [1] | Karam, M. C., Merhbi, S. S., & Ghalayini, W. M. (2013). Rifampicin-induced adrenal insufficiency. International Journal of Tuberculosis and Lung Disease, 17(6), 836-838. |
| [2] | Spencer Ramon Campbell, Ryan M Tierney, Jonea Lim, FRI215 Rifampin Induced Adrenal Insufficiency, Journal of the Endocrine Society, Volume 7, Issue Supplement_1, October-November 2023, bvad114.210, https://doi.org/10.1210/jendso/bvad114.210 |
[1, 2]
. This pharmacological property can lead to adrenal insufficiency in susceptible individuals, resulting in an inadequate physiological response during stress or illness.
On the other hand, tuberculosis (TB) itself is a recognized cause of adrenal insufficiency through direct adrenal involvement, referred to as TB adrenalitis. TB adrenalitis is generally associated with granulomatous destruction of adrenal tissue, particularly in disseminated or severe forms of the disease. Histologically, it is characterized by caseating granulomatous destruction of functional adrenal tissue
| [4] | Jonatan D Lindh, Jekaterina Patrova, R Louise Rushworth, Buster Mannheimer, Henrik Falhammar, Tuberculosis of Adrenal Glands—A Population-based Case-control Study, Journal of the Endocrine Society, Volume 7, Issue 5, May 2023, bvad047, https://doi.org/10.1210/jendso/bvad047 |
| [5] | Gupta S, Ansari MAM, Gupta AK, Chaudhary P, Bansal LK. Current Approach for Diagnosis and Treatment of Adrenal Tuberculosis-Our Experience and Review of Literature. Surg J (N Y). 2022 Mar 3; 8(1): e92-e97. https://doi.org/10.1055/s-0042-1743523 |
| [6] | Hao Huang, Liang Gao, YaDong Li, Wei Tan, Hao Wu, Ye Yuan, Chuan Liu; Adrenal Tuberculosis: A Case Report and Literature Review. Urol Int 8 September 2023; 107 (8): 807–813. https://doi.org/10.1159/000529711 |
[4-6]
. While both rifampicin and TB adrenalitis result in adrenal insufficiency in different pathophysiological mechanisms, their clinical presentation is often indistinguishable, manifesting as hypotension, fatigue, hyponatremia, and hyperkalemia
| [7] | Yokoyama T, Toda R, Kimura Y, Mikagi M, Aizawa H. Addison's disease induced by miliary tuberculosis and the administration of rifampicin. Intern Med. 2009; 48(15): 1297-300. https://doi.org/10.2169/internalmedicine.48.1974 Epub 2009 Aug 3. |
[7]
.
Differentiating rifampicin induced adrenal insufficiency from TB adrenalitis is critical as their management strategies differ. TB adrenalitis necessitates continuation of anti-TB therapy alongside glucocorticoid replacement, as steroid therapy addresses both adrenal insufficiency and the inflammatory sequelae of TB. Conversely, managing rifampicin induced adrenal insufficiency requires discontinuation of rifampicin and initiation of glucocorticoid replacement
| [5] | Gupta S, Ansari MAM, Gupta AK, Chaudhary P, Bansal LK. Current Approach for Diagnosis and Treatment of Adrenal Tuberculosis-Our Experience and Review of Literature. Surg J (N Y). 2022 Mar 3; 8(1): e92-e97. https://doi.org/10.1055/s-0042-1743523 |
| [8] | Jong Sik Kang, Gwang Beom Ko, Jae June Lee, Minsoo Kim, Sung Jin Jeon, Gwang Hyeon Choi, Sun Mok Kim, Woo Je Lee Journal of Yeungnam Medical Science 2012; 29(1): 19-23. https://doi.org/10.12701/yujm.2012.29.1.19 Published online: June 30, 2012. |
[5, 8]
.
The literature extensively documents TB adrenal involvement, whereas reports on rifampicin remain sparse, with only a few cases described globally. This paucity of data may be attributed to underdiagnosis or the absence of routine adrenal function monitoring during TB treatment, particularly in patients receiving rifampicin-based combination therapies. Contributing factors may include the co-administration of other enzyme-inducing drugs, pre-existing adrenal disorders, or a severe TB disease burden. Critically ill patients with a high TB burden are especially at risk and warrant heightened vigilance regarding their adrenal function to facilitate timely diagnosis and management.
| [9] | Yee, T. W.; Mathews, G. J.; Subramaniam, S. D..; Abdullah, N. R. A.; Merican, N. S. Y. A. RIFAMPIN-INDUCED ADRENAL CRISIS. J ASEAN Fed Endocr Soc 2024, 39, 13. |
[9]
.
Current guidelines lack specific recommendations for adrenal function assessment during TB therapy. Incorporating routine evaluation of adrenal function through serum cortisol levels or Adrenocorticotropic hormone (ACTH) stimulation tests could aid in early detection of rifampicin induced adrenal insufficiency. Moreover, prospective studies are needed to establish the incidence of rifampicin induced adrenal insufficiency and evaluate potential risk factors to guide clinical practice
| [12] | Beuschlein, F., Else, T., Bancos, I., Hahner, S., Hamidi, O., van Hulsteijn, L., Husebye, E. S., Karavitaki, N., Prete, A., Vaidya, A., Yedinak, C., & Dekkers, O. M. (2024). European Society of Endocrinology and Endocrine Society Joint Clinical Guideline: Diagnosis and therapy of glucocorticoid-induced adrenal insufficiency. European Journal of Endocrinology, 190(5), G25–G51. https://doi.org/10.1093/EJENDO/LVAE029 |
| [13] | Bornstein, Stefan R et al. “Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline.” The Journal of clinical endocrinology and metabolism vol. 101, 2 (2016): 364-89. https://doi.org/10.1210/jc.2015-1710 |
[12, 13]
.
In this case, the patient's cortisol level of 322 nmol/L (250–650 nmol/L) was within the normal range, which was inappropriately low for his acute stressful situation. This should be confirmed with serum ACTH levels and response to ACTH stimulation test
| [8] | Jong Sik Kang, Gwang Beom Ko, Jae June Lee, Minsoo Kim, Sung Jin Jeon, Gwang Hyeon Choi, Sun Mok Kim, Woo Je Lee Journal of Yeungnam Medical Science 2012; 29(1): 19-23. https://doi.org/10.12701/yujm.2012.29.1.19 Published online: June 30, 2012. |
[8]
.
In conclusion, this case serves as a reminder for clinicians to maintain a high level of vigilance of adrenal insufficiency in patients receiving rifampicin, particularly those exhibiting suggestive symptoms. Regular monitoring of adrenal function in at-risk patients is crucial for timely diagnosis and effective management, ultimately improving patient outcomes. Future studies should focus on establishing clear guidelines for screening and management of this potential complication in patients undergoing TB treatment. The world literature revealed that adrenal insufficiency is commonly present in chronically ill patients; hence, extra vigilance is mandatory in the management of such patients to promptly diagnose and treat this condition, preventing potential complications
| [9] | Yee, T. W.; Mathews, G. J.; Subramaniam, S. D..; Abdullah, N. R. A.; Merican, N. S. Y. A. RIFAMPIN-INDUCED ADRENAL CRISIS. J ASEAN Fed Endocr Soc 2024, 39, 13. |
| [10] | Jafari S, Behjati J, Shafaei K, Dehghan Manshadi SA, Seifi A. Adrenal function in patients receiving rifampin-based anti-tuberculosis regimens: A cross-sectional study in Iran. Caspian J Intern Med. 2020 Fall; 11(4): 458-459. https://doi.org/10.22088/cjim.11.4.458 |
| [11] | Sarin BC, Sibia K, Kukreja S. Study of adrenal function in patients with tuberculosis. Indian J Tuberc. 2018; 65: 241–5. https://doi.org/10.1016/j.ijtb.2017.08.033 |
[9-11]
.
Abbreviations
TB | Tuberculosis |
AFB | Acid-fast Bacillus |
ECG | Electrocardiogram |
CTPA | Computed Tomography Pulmonary Angiography |
USS | Ultrasound Scan |
Author Contributions
Dushantha Madegedara: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing
Dhananjaya Ranathunga: Data curation, Formal Analysis, Investigation, Writing – review & editing
Dilky Hirushika Madegedara Rathnayake: Data curation, Formal Analysis, Project administration, Visualization
Damith Nissanka: Conceptualization, Data curation, Formal Analysis, Methodology, Software, Validation, Writing – review & editing
Conflict of Interest
The authors declare no conflicts of interest.
References
| [1] |
Karam, M. C., Merhbi, S. S., & Ghalayini, W. M. (2013). Rifampicin-induced adrenal insufficiency. International Journal of Tuberculosis and Lung Disease, 17(6), 836-838.
|
| [2] |
Spencer Ramon Campbell, Ryan M Tierney, Jonea Lim, FRI215 Rifampin Induced Adrenal Insufficiency, Journal of the Endocrine Society, Volume 7, Issue Supplement_1, October-November 2023, bvad114.210,
https://doi.org/10.1210/jendso/bvad114.210
|
| [3] |
Mukhtar, A., & Khan, A. (2020). Adverse drug reactions associated with anti-tuberculosis drugs: A review. Journal of Infection and Public Health, 13(1), 19-24.
https://doi.org/10.1016/j.jiph.2019.03.015
|
| [4] |
Jonatan D Lindh, Jekaterina Patrova, R Louise Rushworth, Buster Mannheimer, Henrik Falhammar, Tuberculosis of Adrenal Glands—A Population-based Case-control Study, Journal of the Endocrine Society, Volume 7, Issue 5, May 2023, bvad047,
https://doi.org/10.1210/jendso/bvad047
|
| [5] |
Gupta S, Ansari MAM, Gupta AK, Chaudhary P, Bansal LK. Current Approach for Diagnosis and Treatment of Adrenal Tuberculosis-Our Experience and Review of Literature. Surg J (N Y). 2022 Mar 3; 8(1): e92-e97.
https://doi.org/10.1055/s-0042-1743523
|
| [6] |
Hao Huang, Liang Gao, YaDong Li, Wei Tan, Hao Wu, Ye Yuan, Chuan Liu; Adrenal Tuberculosis: A Case Report and Literature Review. Urol Int 8 September 2023; 107 (8): 807–813.
https://doi.org/10.1159/000529711
|
| [7] |
Yokoyama T, Toda R, Kimura Y, Mikagi M, Aizawa H. Addison's disease induced by miliary tuberculosis and the administration of rifampicin. Intern Med. 2009; 48(15): 1297-300.
https://doi.org/10.2169/internalmedicine.48.1974
Epub 2009 Aug 3.
|
| [8] |
Jong Sik Kang, Gwang Beom Ko, Jae June Lee, Minsoo Kim, Sung Jin Jeon, Gwang Hyeon Choi, Sun Mok Kim, Woo Je Lee Journal of Yeungnam Medical Science 2012; 29(1): 19-23.
https://doi.org/10.12701/yujm.2012.29.1.19
Published online: June 30, 2012.
|
| [9] |
Yee, T. W.; Mathews, G. J.; Subramaniam, S. D..; Abdullah, N. R. A.; Merican, N. S. Y. A. RIFAMPIN-INDUCED ADRENAL CRISIS. J ASEAN Fed Endocr Soc 2024, 39, 13.
|
| [10] |
Jafari S, Behjati J, Shafaei K, Dehghan Manshadi SA, Seifi A. Adrenal function in patients receiving rifampin-based anti-tuberculosis regimens: A cross-sectional study in Iran. Caspian J Intern Med. 2020 Fall; 11(4): 458-459.
https://doi.org/10.22088/cjim.11.4.458
|
| [11] |
Sarin BC, Sibia K, Kukreja S. Study of adrenal function in patients with tuberculosis. Indian J Tuberc. 2018; 65: 241–5.
https://doi.org/10.1016/j.ijtb.2017.08.033
|
| [12] |
Beuschlein, F., Else, T., Bancos, I., Hahner, S., Hamidi, O., van Hulsteijn, L., Husebye, E. S., Karavitaki, N., Prete, A., Vaidya, A., Yedinak, C., & Dekkers, O. M. (2024). European Society of Endocrinology and Endocrine Society Joint Clinical Guideline: Diagnosis and therapy of glucocorticoid-induced adrenal insufficiency. European Journal of Endocrinology, 190(5), G25–G51.
https://doi.org/10.1093/EJENDO/LVAE029
|
| [13] |
Bornstein, Stefan R et al. “Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline.” The Journal of clinical endocrinology and metabolism vol. 101, 2 (2016): 364-89.
https://doi.org/10.1210/jc.2015-1710
|
Cite This Article
-
APA Style
Madegedara, D., Ranathunga, D., Rathnayake, D. H. M., Nissanka, D. (2025). Uncommon Life-threatening Complication of Anti Tuberculosis Treatment. Science Journal of Public Health, 13(1), 12-16. https://doi.org/10.11648/j.sjph.20251301.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Madegedara, D.; Ranathunga, D.; Rathnayake, D. H. M.; Nissanka, D. Uncommon Life-threatening Complication of Anti Tuberculosis Treatment. Sci. J. Public Health 2025, 13(1), 12-16. doi: 10.11648/j.sjph.20251301.12
Copy
|
Download
AMA Style
Madegedara D, Ranathunga D, Rathnayake DHM, Nissanka D. Uncommon Life-threatening Complication of Anti Tuberculosis Treatment. Sci J Public Health. 2025;13(1):12-16. doi: 10.11648/j.sjph.20251301.12
Copy
|
Download
-
@article{10.11648/j.sjph.20251301.12,
author = {Dushantha Madegedara and Dhananjaya Ranathunga and Dilky Hirushika Madegedara Rathnayake and Damith Nissanka},
title = {Uncommon Life-threatening Complication of Anti Tuberculosis Treatment},
journal = {Science Journal of Public Health},
volume = {13},
number = {1},
pages = {12-16},
doi = {10.11648/j.sjph.20251301.12},
url = {https://doi.org/10.11648/j.sjph.20251301.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjph.20251301.12},
abstract = {This case report details the occurrence of adrenal insufficiency in a 46-year-old male undergoing anti-tuberculosis (TB) treatment. The patient developed clinical symptoms indicative of adrenal insufficiency on the fourth day following the initiation of anti-Tuberculosis treatment which consisted of rifampicin, a key component of the TB treatment regimen. Initial symptoms at fourth day of treatment included postural dizziness, fatigue, nausea, and abdominal pain. His biochemical investigations revealed hypoglycemia, hyperkalemia, mild metabolic acidosis, and a disproportionately low random cortisol level during the acute presentation. A diagnosis of rifampicin-induced adrenal insufficiency was strongly suspected, supported by clinical presentation and the temporal relationship to therapy initiation. The patient was subsequently transferred to the intensive care unit and his condition improved only after initiating, administering of hydrocortisone and discontinuing rifampicin therapy. Following stabilization, an alternative anti-TB regimen excluding rifampicin was introduced. The patient showed gradual clinical improvement with hydrocortisone therapy and continued TB treatment. The report discusses clinical presentation, diagnostic evaluation, management, and the importance of recognizing this potential life-threatening adverse effect providing insight into the critical need for increased awareness and early recognition of adrenal insufficiency as a rare but potentially life-threatening complication of anti-tuberculosis therapy, extending the importance to guiding clinical vigilance and treatment protocols. This case serves an important reference and supports the routine monitoring of adrenal function during rifampicin therapy to guide future clinical practice.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Uncommon Life-threatening Complication of Anti Tuberculosis Treatment
AU - Dushantha Madegedara
AU - Dhananjaya Ranathunga
AU - Dilky Hirushika Madegedara Rathnayake
AU - Damith Nissanka
Y1 - 2025/01/14
PY - 2025
N1 - https://doi.org/10.11648/j.sjph.20251301.12
DO - 10.11648/j.sjph.20251301.12
T2 - Science Journal of Public Health
JF - Science Journal of Public Health
JO - Science Journal of Public Health
SP - 12
EP - 16
PB - Science Publishing Group
SN - 2328-7950
UR - https://doi.org/10.11648/j.sjph.20251301.12
AB - This case report details the occurrence of adrenal insufficiency in a 46-year-old male undergoing anti-tuberculosis (TB) treatment. The patient developed clinical symptoms indicative of adrenal insufficiency on the fourth day following the initiation of anti-Tuberculosis treatment which consisted of rifampicin, a key component of the TB treatment regimen. Initial symptoms at fourth day of treatment included postural dizziness, fatigue, nausea, and abdominal pain. His biochemical investigations revealed hypoglycemia, hyperkalemia, mild metabolic acidosis, and a disproportionately low random cortisol level during the acute presentation. A diagnosis of rifampicin-induced adrenal insufficiency was strongly suspected, supported by clinical presentation and the temporal relationship to therapy initiation. The patient was subsequently transferred to the intensive care unit and his condition improved only after initiating, administering of hydrocortisone and discontinuing rifampicin therapy. Following stabilization, an alternative anti-TB regimen excluding rifampicin was introduced. The patient showed gradual clinical improvement with hydrocortisone therapy and continued TB treatment. The report discusses clinical presentation, diagnostic evaluation, management, and the importance of recognizing this potential life-threatening adverse effect providing insight into the critical need for increased awareness and early recognition of adrenal insufficiency as a rare but potentially life-threatening complication of anti-tuberculosis therapy, extending the importance to guiding clinical vigilance and treatment protocols. This case serves an important reference and supports the routine monitoring of adrenal function during rifampicin therapy to guide future clinical practice.
VL - 13
IS - 1
ER -
Copy
|
Download